ONE
INTRODUCTION
Most
writers on ophthalmology appear to believe that the last word about
problems of refraction has been spoken, and from their viewpoint the
last word is a very depressing one. Practically everyone in these
days suffers from some form of refractive error. Yet we are told that
for these ills, which are not only so inconvenient, but often so
distressing and dangerous, there is not only no cure, and no
palliatives save those optic crutches known as eyeglasses, but, under
modern conditions of life, practically no prevention.
It
is a well known fact that the human body is not a perfect mechanism.
Nature, in the evolution of the human tenement, has been guilty of
some maladjustments. She has left, for instance, some troublesome
bits of scaffolding, like the vermiform appendix, behind. But nowhere
is she supposed to have blundered so badly as in the construction of
the eye. With one accord ophthalmologists tell us that the visual
organ of man was never intended for the uses to which it is now put.
Eons before there were any schools or printing presses, electric
lights or moving pictures, its evolution was complete. In those days
it served the needs of the human animal perfectly. Man was a hunter,
a herdsman, a farmer, a fighter. He needed, we are told, mainly
distant vision; and since the eye at rest is adjusted for distant
vision, sight is supposed to have been ordinarily as passive as the
perception of sound, requiring no muscular action whatever. Near
vision, it is assumed, was the exception, necessitating a muscular
adjustment of such short duration that it was accomplished without
placing any appreciable burden upon the mechanism of accommodation.
The fact that primitive woman was a seamstress, an embroiderer,
a weaver, an artist in all sorts of fine and beautiful work, appears
to have been generally forgotten. Yet women living under primitive
conditions have just as good eyesight as the men.
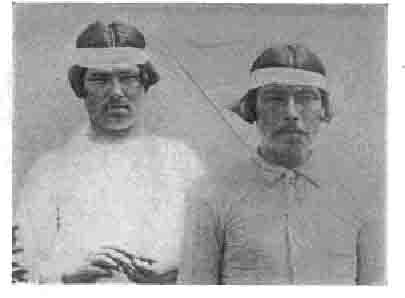
Fig.
1. Pantagonians -- The sight of this primitive pair and of
the following groups of primitive people was tested at the World's
Fair in St. Louis and found to be normal. The unaccustomed experience
of having their pictures taken, however, has evidently so disturbed
them that they were all, probably, myopic when they faced the camera.
(see Chapter IX.)
When
man learned how to communicate his thoughts to others by means of
written and printed forms, there came some undeniably new demands
upon the eye, affecting at first only a few people, but gradually
including more and more, until now, in the more advanced countries,
the great mass of the population is subjected to their influence. A
few hundred years ago even princes were not taught to read and write.
Now we compel everyone to go to school, whether he wishes to or not,
even the babies being sent to kindergarten. A generation or so ago
books were scarce and expensive. To-day, by means of libraries of all
sorts, stationary and traveling, they have been brought within the
reach of practically everyone. The modern newspaper, with its endless
columns of badly printed reading matter, was made possible only by
the discovery of the art of manufacturing paper from wood, which is
a-thing of yesterday. The tallow candle has been but lately displaced
by the various forms of artificial lighting, which tempt most of us
to prolong our vocations and avocations into hours when primitive man
was forced to rest, and within the last couple of decades has come
the moving picture to complete the supposedly destructive
process.
Was
it reasonable to expect that Nature should have provided for all
these developments, and produced an organ that could respond to the
new demands? It is the accepted belief of ophthalmology to-day
that she could not and did not,(1) and that, while the processes of
civilization depend upon the sense of sight more than upon any
other, the visual organ is but imperfectly fitted for its tasks.
There
are a great number of facts which seem to justify this conclusion.
While primitive man appears to have suffered little from defects
of vision, it is safe to say that of persons over twenty-one living
under civilized conditions nine out of every ten have imperfect
sight, and as the age increases the proportion increases, until at
forty it is almost impossible to find a person free from visual
defects. Voluminous statistics are available to prove these
assertions, but the visual standards of the modern army (2) are all
the evidence that is required.
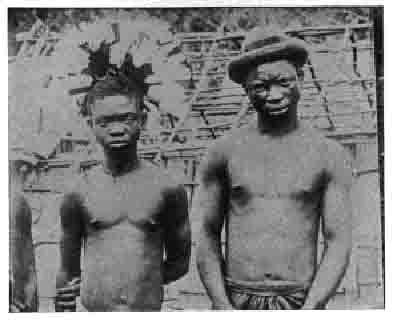
Fig.
2. African Pigmies -- They had normal vision when tested, but
their expressions show that they could not have had it when
photographed.
In
Germany, Austria, France and Italy, vision with glasses determines
acceptance or rejection for military service, and in all these
countries more than six diopters (3) of myopia are allowed, although
a person so handicapped cannot see anything clearly at more than six
inches from his eyes without glasses.
In
the German Army a recruit for general service is required - or was
required under the former government - to have a corrected vision of
6/12 in one eye. That is, he must be able to read with this eye at
six metres the line normally read at twelve metres. In other words,
he is considered fit for military service if the vision of one eye
can be brought up to one-half normal with glasses. The vision in the
other eye may be minimal, end in the Landsturm one eye may be blind.
Incongruous as the eyeglass seems upon the soldier, military
authorities upon the European continent have come to the conclusion
that a man with 6/12 vision wearing glasses is more serviceable than
a man with 6/24 vision (one-quarter normal) without them.
In
Great Britain it was formerly uncorrected vision that determined
acceptance or rejection for military service. This was probably due
to the fact that previous to the recent war the British Army was used
chiefly for foreign service, at such distances from its base that
there might have been difficulty in providing glasses. The standard
at the beginning of the war was 6/24 (uncorrected) for the better eye
and 6/60 (uncorrected) for the poorer, which was required to be the
left. Later, owing to the difficulty of securing enough men with even
this moderate degree of visual acuity, recruits were accepted whose
vision in the right eye could be brought up to 6/12 by correction,
provided the vision of one eye was 6/24 without correction.(4)
Up
to 1908 the United States required normal vision in recruits for its
military service. In that year Bannister and Shaw made some
experiments from which they concluded that a perfectly sharp image of
the target was not necessary for good shooting, and that, therefore,
a visual acuity of 20/40 (the equivalent in feet of 6/12 in metres),
or even 20/70, in the aiming eye only, was sufficient to make an
efficient soldier. This conclusion was not accepted without protest,
but normal vision had become so rare that it probably seemed to those
in authority that there was no use insisting upon it; and the visual
standard for admission
to the Army was accordingly lowered to 20/40 for the better eye and
20/100 for the poorer, while it was further provided that a recruit
might be accepted when unable with the better eye to read all the
letters on the 20/40 line, provided he could read some of the letters
on the 20/30 line.(5)

Fig.
3. Moros from the Phillippines.
With sight ordinarily normal all were probably myopic when
photographed except
the one at the upper left whose eyes are shut.
In
the first enrollment of troops for the European war it is a matter of
common knowledge that these very low standards were found to be too
high and were interpreted with great liberality. Later they were
lowered so that men might be "unconditionally accepted for
general military service" with a vision of 20/100 in each eye
without glasses, provided that the sight of one eye could be brought
up to 20/40 with glasses, while for limited service 20/200 in each
eye was sufficient, provided the vision of one eye might be brought
up to 20/40 with glasses.(6) Yet 21.68 per cent of all rejections in
the first draft, 13 per cent more than for any other single cause,
were for eye defects,<(7) while under the revised standards these
defects still constituted one of three leading causes of rejection.
They were responsible for 10.65 per cent of the rejections, while
defects of the bones and joints and of the heart and bloodvessels
ran, respectively, about two and two and a half per cent higher.(8)
For
more than a hundred years the medical profession has been seeking for
some method of checking the ravages of civilization upon the human
eye. The Germans, to whom the matter was one of vital military
importance, have spent millions of dollars in carrying out the
suggestions of experts, but without avail; and it is now admitted by
most students of the subject that the methods which were once
confidently advocated as reliable safeguards for the eyesight of our
children - have accomplished little or nothing. Some take a more
cheerful view of the matter, but their conclusions are hardly borne
out by the army standards just quoted.
For
the prevailing method of treatment, by means of compensating lenses,
very little was ever claimed except that these contrivances
neutralized the effects of the various conditions for which they were
prescribed, as a crutch enables a lame man to walk. It has also been
believed that they sometimes checked the progress of these
conditions; but every ophthalmologist now knows that their usefulness
for this purpose, if any, is very limited. In the case of
myopia(9)
(shortsight), Dr. Sidler-Huguenin of Zurich, in a striking paper
recently published,(10) expresses the opinion that glasses and all
methods now at our command are "of but little avail" in
preventing either the progress of the error of refraction, or the
development of the very serious complications with which it is often
associated.
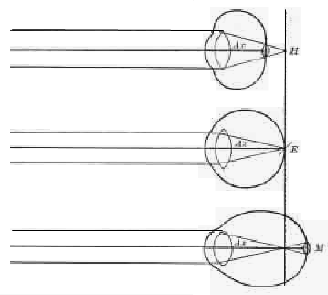
Fig.
4. Diagram of Hypermetropic, Emmetropic and Myopic Eyeballs
H, hypermetropia; E, emmetropia; M, myopia; Ax, optic axis. Note that
in hyper-metropia and myopia the rays, instead of coming to a focus,
form a round spot upon the retina.
These
conclusions are based on the study of thousands of cases in Dr.
Huguenin's private practice and in the clinic of the University of
Zurich, and regarding one group of patients, persons connected with
the local educational institutions, he states that the failure took
place in spite of the fact that they followed his instructions for
years "with the greatest energy and pertinacity," sometimes
even changing their professions.
I
have been studying the refraction of the human eye for more than
thirty years, and my observations fully confirm the foregoing
conclusions as to the uselessness of all the methods heretofore
employed for the prevention and treatment of errors of refraction. I
was very early led to suspect, however, that the problem was by no
means an unsolvable one
Every
ophthalmologist of any experience knows that
the
theory of the incurability of errors of refraction does not fit
the observed facts. Not infrequently such cases recover
spontaneously, or change from one form to another. It has long been
the custom either to ignore these troublesome facts, or to explain
them away, and fortunately for those who consider it necessary to
bolster up the old theories at all costs, the role attributed to the
lens in accommodation offers, in the majority of cases, a plausible
method of explanation. According to this theory, which most of us
learned at school, the eye changes its focus for vision at different
distances by altering the curvature of the lens; and in seeking for
an explanation for the inconstancy of the theoretically constant
error of refraction the theorists hit upon the very ingenious idea of
attributing to the lens a capacity for changing its curvature, not
only for the purpose of normal accommodation, but to cover up or to
produce accommodative errors. In hypermetropia1(11) - commonly
but improperly called farsight, although the patient with such a
defect can see clearly neither at the distance nor the nearpoint -
the eyeball is too short from the front backward, and all rays of
light, both the convergent ones coming from near objects, and the
parallel ones coming from distant objects, are focussed behind the
retina, instead of upon it. In myopia it is too long, and while the
divergent rays from near objects come to a point upon the retina, the
parallel ones from distant objects do not reach it. Both these
conditions are supposed to be permanent, the one congenital, the
other acquired. When, therefore, persons who at one time appear to
have hypermetropia, or myopia, appear at other times not to have
them, or to have them in lesser degrees, it is not permissible to
suppose that there has been a change in the shape of the eyeball.
Therefore, in the case of the disappearance or lessening of
hypermetropia, we are asked to believe that the eye, in the act of
vision, both at the near-point and at the distance, increases the
curvature of the lens sufficiently to compensate, in whole or in
part, for the flatness of the eyeball. In myopia, on the contrary, we
are told that the eye actually goes out of its way to produce the
condition, or to make an existing condition worse. In other words,
the so-called "ciliary muscle," believed to control the
shape of the lens, is credited with a capacity for getting into a
more or less continuous state of contraction, thus keeping the lens
continuously in a state of convexity which, according to the theory,
it ought to assume only for vision at the nearpoint. These curious
performances may seem unnatural to the lay mind; but ophthalmologists
believe the tendency to indulge in them to be so ingrained in the
constitution of the organ of vision that, in the fitting of glasses,
it is customary to instill atropine - the "drops" with
which everyone who has ever visited an oculist is familiar - into the
eye, for the purpose of
paralyzing the ciliary muscle and thus, by preventing any change of
curvature in the lens, bringing out "latent hypermetropia"
and getting rid of "apparent myopia."
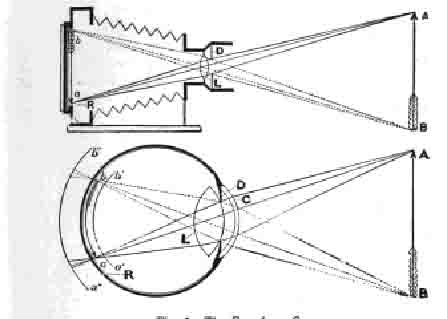
Fig.
5. The Eye As a Camera -- The photographic apparatus:
D, diaphragm made of circular overlapping plates of metal by
means of which the opening through which the rays of light enter the
chamber can be enlarged or contracted-L, lens; R, sensitive
plate (the retina of the eye); AB, object to be photographed; ab,
image on the sensitive plate._______________________________________
The
interference of the lens, however, is believed to account for only
moderate degrees of variation in errors of refraction, and that only
during the earlier years of life. For the higher ones, or those that
occur after forty-five years of age, when the lens is supposed to
have lost its elasticity to a greater or less degree, no
plausible explanation has ever been devised. The disappearance
of astigmatism, (12) or changes in its character, present an
even more baffling problem. Due in most cases to an
unsymmetrical change in the curvature of the cornea, and resulting
in failure to bring the light rays to a focus at any point, the eye
is supposed to possess only a limited power of overcoming this
condition; and yet astigmatism comes and goes with as much facility
as do other errors of refraction. It is well known, too, that it can
be produced voluntarily. Some persons can produce as much as
three diopters. I myself can produce one and a half.
Examining
30,000 pairs of eyes a year at the New York Eye and Ear Infirmary and
other institutions, I observed many cases in which errors of
refraction either recovered spon-taneously, or changed their form,
and I was unable either to ignore them, or to satisfy myself with the
orthodox explanations, even where such explanations were
available. It seemed to me that if a statement is a truth it
must always be a truth. There can be no exceptions. If errors of
refraction are incurable, they should not recover, or change their
form, spontaneously.
In
the course of time I discovered that myopia and hypermetropia, like
astigmatism, could be produced at will; that myopia was not, as
we have so long believed, associated with the use of the eyes at
the near-point, but with a strain to see distant objects, strain at
the near-point being associated with hypermetropia; that no error of
refraction was ever a constant condition; and that the lower
degrees of refractive error were curable, while higher degrees
could be improved.
In
seeking for light upon these problems I examined tens of
thousands of eyes, and the more facts I accumulated the more
difficult it became to reconcile them with the accepted views.
Finally,
about half a dozen years ago, I undertook a series of observations
upon the eyes of human beings and the lower animals the results of
which convinced both myself and others that the lens is not a factor
in accommodation, and that the adjustment necessary for vision
at different distances is affected in the eye, precisely as it
is in the camera, by a change in the length of the organ, this
alteration being brought about by the action of the muscles on the
outside of the globe.
Equally convincing was the demonstration that errors of refraction,
including presbyopia, are due, not to an organic change in the shape
of the eyeball, or in the constitution of the lens, but to a
functional and therefore curable derangement in the action of the
extrinsic muscles.
In
making these statements I am well aware that I am controverting the
practically undisputed teaching of ophthalmological
science for the better part of a century; but I have been driven
to the conclusions which they embody by the facts, and that so slowly
that I am now surprised at my own blindness. At the time I was
improving high degrees of myopia; but I wanted to be conservative,
and I differentiated between functional myopia, which I was able
to cure, or improve, and organic myopia, which, in deference to the
orthodox tradition, I accepted as incurable.
Fig.
6. Mexican Indians -- With normal sight when tested all the
members of this primitive group are now either squinting or staring.

Fig.
7. Ainus, the Aboriginal Inhabitants of Japan -- All show signs
of temporary imperfect sight.
CITATIONS
1.
The unnatural strain of accommodating the eyes to close work (for
which they were not intended) leads to myopia in a large proportion
of growing children - Rosenau Preventive Medicine and Hygiene, third
edition, 1917, p. 1093.
The
compulsion of fate as well as an error of evolution has brought it
about that the unaided eye must persistently struggle against the
astonishing difficulties and errors inevitable in its structure
function and circumstance - Gould The Cause, Nature and Consequences
of Eyestrain, Pop Sci Monthly, Dec., 1905.
With
the invention of writing and then with the invention of the
printing-press a new element was introduced, and one evidently not
provided for by the process of evolution The human eye which had been
evolved for distant vision is being forced to perform a new part, one
for which it had not been evolved, and for which it is poorly adapted
The difficulty is being daily augmented - Scott The Sacrifice of the
Eyes of School Children, Pop Sci Monthly, Oct., 1907
2.
Ford Details of Military Medical Administration published with the
approval of the Surgeon General, U.S. Army, second revised edition,
1918, pp. 498-499.
3.
A diopter is the focussing power necessary to bring parallel rays to
a focus at one metre.
4.
Tr. Ophth. Soc. U. Kingdom, vol. xxxviii, 1918, pp. 130-131.
5.
Harvard Manual of Military Hygiene for the Military Services of the
United States, published under the authority and with the approval of
the Surgeon General, U. S. Army third revised edition, 1917, p. 195.
6.
Standards of Physical Examination for the Use of Local Boards,
District Boards, and Medical Advisory Boards under the Selective
Service
Regulations,
issued through the office of the Provost Marshal General, 1918.
7.
Report of the Provost Marshal General to the Secretary of War on the
First Draft under the Selective Service Act, 1917.
8.
Second Report of the Provost Marshal General to the Secretary of War
on the Operations of the Selective Service System to December 20,
1918.
9.
From the Greek myein, to close, and ops, the eye, literally a
condition in which the subject closes the eye, or blinks.
10.
Archiv f Augenh, vol. lxxix, 1915, translated in Arch. Ophth., vol.
xlv, No. 6, Nov., 1916.
11.
From the Greek hyper, over, rnetrors, measure, and ops, the eye.
12.
From the Greek a, without, and stigma, a point.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
II
SIMULTANEOUS RETINOSCOPY
Much
of my information about the eyes has been obtained by means of
simultaneous retinoscopy. The retinoscope is an instrument used
to measure the refraction of the eye. It throws a beam of light into
the pupil by reflection from a mirror,; the light being either
outside the instrument - above and behind the subject - or
arranged within it by means of an electric battery. On looking
through the sight-hole one sees a larger or smaller part of the pupil
filled with light, which in normal human eyes is a reddish yellow,
because this is the color of the retina, but which is green in a
cat's eye, and might be white if the retina were diseased. Unless the
eye is exactly focussed at the point from which it is being observed,
one sees also a dark shadow at the edge of the pupil, and it is the
behavior of this shadow when the mirror is moved in various
directions which reveals the refractive condition of the eye. If the
instrument is used at a distance of six feet or more, and the shadow
moves in a direction opposite to the movement of the mirror, the eye
is myopic. If it moves in the same direction as the mirror, the eye
is either hypermetropic or normal; but in the case of hypermetropia
the movement is more pronounced than in that of normality, and
an expert can usually tell the difference between the two states
merely by the nature of the movement. In astigmatism the movement is
different in different meridians. To determine the degree of the
error, or to distinguish accurately between hypermetropia
and normality, or between the different kinds of astigmatism, it is
usually necessary to place a glass before the eye of the subject. If
the mirror is concave instead of plane, the movements described
will be reversed; but the plane mirror is the one most commonly used.
Fig.
8. The Usual Method of Using the Retinoscope -- The observer is
so near the subject that the latter is made nervous, and this changes
the refraction.
This
exceedingly useful instrument has possibilities which have not
been generally realized by the medical profession. Most
ophthalmologists depend upon the Snellen' test card,
supplemented by trial lenses, to determine whether the
vision is normal or not, and to determine the degree of any
abnormality that may exist. This is a slow, awkward and unreliable
method of testing the vision, and absolutely unavailable for the
study of the refraction of the lower animals, of infants, and of
adult human beings under the conditions of life.
The
test card and trial lenses can be used only under certain favorable
conditions, but the retinoscope can be used anywhere. It is a little
easier to use it in a; dim light than in a bright one, but it may be
used in any light, even with the strong light of the sun shining
directly into the eye. It may also be used under many other
unfavorable conditions.
It
takes a considerable time, varying from minutes to hours, to measure
the refraction with the Snellen test card and trial lenses. With the
retinoscope, however, it can be determined in a fraction of a
second. By the former method it would be impossible, for instance, to
get any information about the refraction of a baseball player at the
moment he swings for the ball, at the moment he strikes it, and at
the moment after he strikes it. But with the retinoscope it is quite
easy to determine whether his vision is normal, or whether he is
myopic, hypermetropic, or astigmatic, when he does these things;
and if any errors of refraction are noted, one can guess their degree
pretty accurately by the rapidity of the movement of the shadow.
With
the Snellen test card and trial lenses conclusions must be drawn from
the patient's statements as to what he sees; but the patient often
becomes so worried and confused during the examination that he does
not know what he sees, or whether different glasses make his sight
better or worse; and, moreover, visual acuity is not reliable
evidence of the state of the refraction. One patient with two
diopters of myopia may see twice as much as another with the same
error of refraction. The evidence of the test card is, in fact,
entirely subjective; that of the retinoscope is entirely objective,
depending in no way upon the statements of the patient.
In
short, while the testing of the refraction by means of the Snellen
test card and trial lenses requires considerable time, and can be
done only under certain artificial conditions, with results that are
not always reliable, the retinoscope can be used under all sorts
of normal and abnormal conditions on the eyes both of human beings
and the lower animals; and the results, when it is used properly, can
always be depended upon. This means that it must not be brought
nearer to the eye than six feet; otherwise the subject will be
made nervous, the refraction, for reasons which will be explained
later, will be changed, and no reliable observations will be
possible. In the case of animals it is often necessary to use it at a
much greater distance.
For
thirty years I have been using the retinoscope to study the
refraction of the eye. With it I have examined the eyes of tens of
thousands of school children, hundreds of infants and thousands
of animals, including cats, dogs, rabbits,
horses,
cows, birds, turtles, reptiles and fish. I have used it when the
subjects were at rest and when they were in motion - also when I
myself was in motion; when they were asleep and when they were awake
or even under ether and chloroform. I have used it in the daytime and
at night, when the subjects were comfortable and when they were
excited; when they were trying to see and when they were not; when
they were lying and when they were telling the truth; when the
eyelids were partly closed, shutting off part of the area of the
pupil, when the pupil was dilated, and also when it was contracted to
a pin-point; when the eye was oscillating from side to side, from
above downward and in other directions. In this way I discovered many
facts which had not previously been known, and which I was quite
unable to reconcile with the orthodox teachings on the subject. This
led me to undertake the series of experiments already alluded
to. The results were in entire harmony with my previous observations,
and left me no choice but to reject the entire body of orthodox
teaching about accommodation and errors of refraction. But before
describing these experiments I must crave the readers patience
while I present a resume of the evidence upon which the accepted
views of accommodation are based. This evidence, it seems to me, is
as strong an argument as any I could offer against the doctrine that
the lens is the agent of accommodation, while an understanding of the
subject is necessary to an understanding of my experiments.
THE CURE OF
IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER III
EVIDENCE FOR THE ACCEPTED THEORY OF ACCOMMODATION
The
power of the eye to change its focus for vision at different
distances has puzzled the scientific mind ever since Kepler(1) tried
to explain it by supposing a change in the position of the
crystalline lens. Later on every imaginable hypothesis was
advanced to account for it. The idea of Kepler had many supporters.
So also had the idea that the change of focus was effected by a
lengthening of the eyeball. Some believed that the contractive power
of the pupil was sufficient to account for the phenomenon,
until the fact was established, by the operation for the removal of
the iris, that the eye accommodated perfectly without this part of
the visual mechanism. Some, dissatisfied with all these
theories, discarded them all, and boldly asserted that no change of
focus took place,(2) a view which was conclusively disproven
when the invention of the ophthalmoscope made it possible to see
the interior of the eye.
Fig.
9. Diagrams of the Images of Purkinje
No.
1. - Images of a candle: a, on the cornea; b, on the front of the
lens- c, on the back of the lens.
No.
2. - Images of lights shining through rectangular openings in a
screen while the eye is at rest (R) and during accommodation
(A): a, on the cornea; b, on the front of the lens; c, on the back of
the lens (after Helmholtz).
Note
that in No. 2, A, the central images are smaller and have approached
each other, a change which, if it actually took place would indicate
an increase of curvature in the front of the lens during
accommodation. ... The idea that the change of focus might be brought
about by a change in the form of the lens appears to have been first
advanced, according to Landolt,(3) by the Jesuit, Scheiner (1619).
Later it was put forward by Descartes (1637). But the first definite
evidence in support of the theory was presented by Dr. Thomas Young
in a paper read before the Royal Society in 1800.(4) "He adduced
reasons," says Donders, "which, properly understood, should
be taken as positive proofs."(5) At the time, however, they
attracted little attention.
About
half a century later it occurred to Maximilian Langenbeck3 to seek
light on the problem by the aid of what are known as the images of
Purkinje.(6) If a small bright light, usually a candle, is held in
front of and a little to one side of the eye, three images are seen:
one bright and upright; another large, but less bright, and also
upright; and a third small, bright and inverted. The first comes from
the cornea, the transparent covering of the iris and pupil, and the
other two from the lens, the upright one from the front and the
inverted one from the back. The corneal reflection was known to the
ancients, although its origin was not discovered till later; but the
two reflections from the lens were first observed in 1823 by
Purkinje; whence the trio of images is now associated with his name.
Langenbeck
examined these images with the naked eye, and reached the conclusion
that during accommodation the middle one became smaller than
when the eye was at rest. And since an image reflected from a convex
surface is diminished in proportion to the convexity of that
surface, he concluded that the front of the lens became more
convex when the eye adjusted itself for near vision. Donders repeated
the experiments of Langenbeck, but was unable to make any
satisfactory observations. He predicted, however, that if the
images were examined with a magnifier they would "show with
certainty" whether the form of the lens changed during
accommodation. Cramer,(7) acting on this suggestion,
examined the images as magnified from ten to twenty times, and thus
convinced himself that the one reflected from the front of the lens
became considerably smaller during accommodation.
Subsequently
Helmholtz, working independently, made a similar observation,
but by a somewhat different method. Like Donders, he found the image
obtained by the ordinary methods on the front of the lens very
unsatisfactory, and in his "Handbook of Physiological
Optics" he describes it as being "usually so blurred that
the form of the flame cannot be definitely distinguished."
(9)(8) So he placed two lights, or one doubled by reflection from a
mirror, behind a screen in which were two small rectangular openings,
the whole being so arranged that the lights shining through the
openings of the screen formed two: images on each of the reflecting
surfaces. During accommodations, it seemed to him that the two
images on the front of the lens became smaller and approached
each other, while on the return of the eye to a state of rest they
grew larger again and separated This change, he said, could be seen
"easily and distinctly."(10) The observations of
Helmholtz regarding the behavior of the lens in accommodation,
published about the middle of the last century, were soon accepted as
facts, and have ever since been stated as such in every text-book
dealing with the subject.
"We
may say," writes Landolt, "that the discovery of the part
played by the crystalline lens in the act of accommodation is one of
the finest achievements of medical physiology, and the theory of its
working is certainly one of the most firmly established; for not only
have "savans" furnished lucid and mathematical proofs of
its correctness, but all other theories which have been advanced as
explaining accommodation have been easily and entirely
overthrown. ...The fact that the eye is accommodated for near vision
by an increase in the curvature of its crystalline lens, is, then,
incontestably proved."(11)
"The
question was decided," says Tscherning, "by the observation
of the changes of the images of Purkinje during accommodation, which
prove that accommodation is effected by an increase of curvature
of the anterior surface of the crystalline lens."(12)
The
greatest thinkers," says Cohn, "have mastered a host
of difficulties in discovering this arrangement, and it is only in
very recent times that its processes have been clearly and perfectly
set forth in the works of Sanson, Helmholtz, Brucke, Hensen and
Volckers."(13)
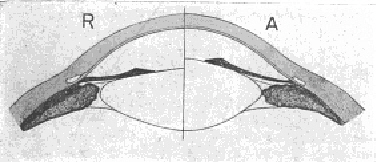
Fig.
10. Diagram by Which Helmholtz Illustrated His Theory of
Accommodation -- R is supposed to be the resting state of
the lens, in which it is adjusted for distant vision. In A the
suspensory ligament is supposed to have been relaxed through the
contraction of the ciliary muscle, permitting the lens to bulge
forward by virtue of its own
elasticity._____________________________________________
Huxley
refers to the observations of Helmholtz as the "facts of
adjustment with which all explanations of that process must
accord,"(14) and Donders calls his theory the "true
principle of accommodation."(15)
Arlt,
who had advanced the elongation theory and believed that no other was
possible, at first opposed the conclusions of Cramer and Helmholtz,
(16) but later accepted them.(17)
Yet
in examining the evidence for the theory we can only wonder at the
scientific credulity which could base such an important department of
medical practice as the treatment of the eye upon such a mass of
contradictions.
Helmholtz,
while apparently convinced of the correctness of his
observations indicating a change of form in the lens during
accommodation, felt himself unable to speak with certainty
of the means by which the supposed change was effected,(18) and
strangely enough the question is still being debated. Finding, as he
states, "absolutely nothing but the ciliary muscle to
which accommodation could be attributed,"(19)
Helmholtz concluded that the changes which he thought he had
observed in the curvature of the lens must be effected by the
action of this muscle; but he was unable to offer any
satisfactory theory of the way it operated to produce these
results, and he explicitly stated that the one he suggested possessed
only the character of probability.

Fig.
11. Thomas Young (1773-1829) --
English physician and man of science who was the first to
present a serious argument in support of the view that accommodation
is brought about by the agency of the lens.
Some
of his disciples, "more loyal than the king," as Tscherning
has pointed out, "have proclaimed as certain what he himself
with much reserve explained as probable,"(20) but there has
been no such unanimity of acceptance in this case as in that of the
observations regarding the behavior of the images reflected from
the lens. No one except the present writer, so far as I am
aware, has ventured to question that the ciliary muscle is the agent
of accommodation; but as to the mode of its operation there is
generally felt to be much need for more light. Since the lens is not
a factor in accommodation, it is not strange that no one
was able to find out how it changed its curvature. It "is"
strange, however, that these difficulties have not in any way
disturbed the universal belief that the lens does change.
When
the lens has been removed for cataract the patient usually appears to
lose his power of accommodation, and not only has to wear a
glass to replace the lost part, but has to put on a stronger glass
for reading. A minority of these cases, however, after they
become accustomed to the new condition, become able to see at the
near-point without any change in their glasses. The existence of
these two classes of cases has been a great stumbling block to
ophthalmology. The first and more numerous appeared to support
the theory of the agency of the lens in accommodation; but the
second was hard to explain away, and constituted at one time, as Dr.
Thomas Young observed, the "grand objection" to this
idea. A number of these cases of apparent change of focus in the
lensless eye having been reported to the Royal Society by competent
observers, Dr. Young, before bringing forward his theory of
accommodation, took the trouble to examine some of them, and
considered himself justified in concluding that an error of
observation had been made. While convinced, however, that in such
eyes the "actual focal distance is totally unchangeable,"
he characterized his own evidence in support of this view as only
"tolerably satisfactory."
At
a later period Donders made some investigations from which he
concluded that, "in aphakia(21) not the slightest trace of
accommodative power remains."(22) Helmholtz expressed
similar views, and von Graefe, although he observed a "slight
residuum" of accommodative power in lensless eyes, did not
consider it sufficient to discredit the theory of Cramer and
Helmholtz.

Herman-
Ludwig Ferdinand von Helmholtz (1821-1894)
-- whose observations
regarding the behavior of images reflected from the front of the lens
are supposed to have demonstrated that the curvature of this body
changes during accommodation._____________________________
It
might be due, he said, to the accommodative action of the iris, and
possibly also to a lengthening of the visual axis through the
action of the external muscles.(23)
For
nearly three-quarters of a century the opinions of these masters
have echoed through ophthalmological literature. Yet it is
to-day a perfectly well-known and undisputed fact that many persons,
after the removal of the lens for cataract, are able to see perfectly
at different distances without any change in their glasses. Every
ophthalmologist of any experience has seen cases of this kind, and
many of them have been reported in the literature.
In
1872, Professor Forster of Breslau, reported(24) a series
of twenty-two cases of apparent accommodation in eyes from which
the lens had been removed for cataract. The subjects ranged in age
from eleven to seventyfour years, and the younger ones had more
accommodative power than the elder.
A
year later Woinow of Moscow (25) reported eleven cases, the
subjects being from twelve to sixty years of age. In 1869 and
1870, respectively, Loring
reported(26) to the New York Ophthalmological Society and the
American Ophthalmological Society the case of a young woman of
eighteen who, without any change in her glasses, read the twenty
line on the Snellen test card at twenty feet and also read diamond
type at from five inches to twenty.
On
October 8, 1894, a patient of Dr. A. E. Davis who appeared to
accommodate perfectly without a lens consented to go before the
New York Ophthalmological Society. "The members,"
Dr. Davis reports, (27) "were divided in their opinion as to how
the patient was able to accommodate for the nearpoint with his
distance glasses on"; but the fact that he could see at this
point without any change in his glasses was not to be disputed.
The
patient was a chef, forty-two years old, and on January 27, 1894, Dr.
Davis had removed a black cataract from his right eye, supplying him
at the same time with the usual outfit of glasses, one to replace the
lens, for distant vision, and a stronger one for reading. In October
he returned, not
because
his eye was not doing well, but because he was afraid he might be
"straining" it. He had discarded his reading glasses after
a few weeks, and had since been using only his distance glasses.
Dr.
Davis doubted the truth of his statements, never having seen such a
case before, but found them, upon investigation, to be quite correct.
With his lensless eye and a convex glass of eleven and a half
diopters, the patient read the ten line on the test card at twenty
feet, and with the same glass, and without any change in its
position, he read fine print at from fourteen to eighteen inches.
Dr.
Davis then presented the case to the Ophthalmological
Society but, as has been stated, he obtained no light from that
source. Four months later, February 4, 1895, the patient still read
20/10 at the distance and his range at the near-point had increased
so that he read diamond type at from eight to twenty-two and a
half inches. Dr. Davis subjected him to numerous tests, and
though unable to find any explanation for his strange
performances, he made some interesting observations. The
results of the tests by which Donders satisfied himself that the
lensless eye possessed no accommodative power were quite
different from those reported by the Dutch authority, and Dr. Davis
therefore concluded that these tests were "wholly inadequate to
decide the question at issue." During accommodation the
ophthalmometer(28) showed that the corneal curvature was changed
and that the cornea moved forward a little. Under scopolamine, a
drug sometimes used instead of atropine to paralyze the ciliary
muscle (1/10 per cent solution every five minutes for thirty-five
minutes, followed by a wait of half an hour), these changes took
place as before; they also took place when the lids were held up.
With the possible influence of lid pressure and of the ciliary
muscle eliminated, therefore, Dr. Davis felt himself bound to
conclude that the changes "must have been produced by
the action of the external muscles." Under scopolamine, also,
the man's accommodation was only slightly affected, the range at
the nearpoint being reduced only two and a half inches.
The
ophthalmometer further showed the patient to have absolutely no
astigmatism. It had showed the same thing about three months after
the operation, but three and a half weeks after it he had four and a
half diopters.
Seeking
further light upon the subject Dr. Davis now subjected to similar
tests a case which had previously been reported by Webster in
the "Archives of Pediatrics."(29) The patient had been
brought to -Dr. Webster at the age of ten with double congenital
cataract. The left lens had been absorbed as the result of
successive needlings, leaving only an opaque membrane, the lens
capsule; while the right, which had not been interfered with, was
sufficiently transparent around the edge to admit of useful vision.
Dr. Webster made an opening in the membrane filling the pupil of the
left eye, after which the vision of this eye, with a glass to
replace the lens, was about equal to the vision of the right eye
without a glass. For this reason Dr. Webster did not think it
necessary to give the patient distance glasses, and supplied him with
reading glasses only - plane glass for the-right eye and convex 16D
for the left. On March 14, 1893, he returned and stated that he had
been wearing his reading glasses all the time. With this glass
it was found that he could read the twenty line of the test card at
twenty feet, and read diamond type easily at fourteen inches.
Subsequently the right lens was removed, after which no accommodation
was observed in this eye.
Two
years later, March 16, 1895, he was seen by Dr. Davis, who found that
the left eye now had an accommodative range of from ten to eighteen
inches. In this case no change was observed in the cornea. The
results of the Donders tests were similar to those of the earlier
case, and under scopolamine the eye accommodated as before, but not
quite so easily. No accommodation was observed in the right eye.
These
and similar cases have been the cause of great embarrassment to those
who feel called upon to reconcile them with the accepted theories.
With the retinoscope the lensless eye can be seen to accommodate; but
the theory of Helmholtz has dominated the ophthalmological mind so
strongly that even the evidence of objective tests was not believed.
The
apparent act of accommodation was said not to be real, and many
theories, very curious and unscientific, have been advanced to
account for it. Davis is of the opinion that "the slight change
in the curvature of the cornea, and its slight advancement observed
in some cases, may, in those cases, account for some of the
accommodative power present, but it is such a small factor that
it may be eliminated entirely, since in some of the most marked cases
of accommodation in aphakial eyes no such changes have been
observed."
The
voluntary production of astigmatism is another stumbling block to the
supporters of the accepted theories, as it involves a change in the
shape of the cornea, and such a change is not compatible with the
idea of an “inextensible”(30) eyeball. It seems to
have given them less trouble, however, than the accommodation of the
lensless eye, because fewer of these cases have been observed and
still fewer have been allowed to get into the literature.
Some
interesting facts regarding one have fortunately been given
by Davis, who investigated it in connection with the corneal changes
noted in the lensless eye. The case was that of a house surgeon at
the Manhattan Eye and Ear Hospital, Dr. C. H. Johnson. Ordinarily
this gentleman had half a diopter of astigmatism in each eye; but he
could, at will, increase this to two diopters in the right eye and
one and a half in the left. He did this many times, in the presence
of a number of members of the hospital staff, and also did it when
the upper lids were held up, showing that the pressure of the lids
had nothing to do with the phenomenon.
Later
he went to Louisville, and here Dr. J. M. Ray, at the suggestion
of Dr. Davis, tested his ability to produce astigmatism under the
influence of scopolamine (four instillations, 1/5 per cent solution).
While the eyes were under the influence of the drug the astigmatism
still seemed to increase, according to the evidence of the
ophthalmometer, to one and a half diopters in the right eye
and one in the left. From these facts, the influence of the lids and
of the ciliary muscle having been eliminated, Dr. Davis
concluded that the change in the cornea was "brought about
mainly by the external muscles." What explanation others offer
for such phenomena I do not know.
CITATIONS
1.
Johannes Kepler (1571-1630). German theologian. astronomer and
physicist. Many facts of physiological optics were either discovered,
or first clearly stated, by him.
2.
Donders: On the Anomalies of Accommodation and Refraction of the
Eye. English translation by Moore, 1864, p. 10. Frans Cornelis
Donders (1818-1889) was professor of physiology and
ophthalmology at the University of Utrecht, and is ranked as one
of the greatest ophthalmologists of all time.
3.
Edmund Landolt (1846-) Swiss ophthalmologist who settled in
Paris in 1874, founding an eye clinic which has attracted many
students.
4.
On the Mechanism of the Eye, Phil. Tr. Roy. Soc., London, 1801.
5.
On the Anomalies of Accommodation and Refraction of the Eye, pp.
10-11.
6.
Maximilian Adolf Langenbeck (1518-1877). Professor of anatomy,
surgery and ophthalmology at Gottingen, from 1846 to 1851. Later
settled in Hanover.
7.
Johannes Evangelista von Purkinje (1787-1869). Professor of
physiology at Breslau and Prague, and the discoverer of many
important physiological facts.
8.
Antonie C. Cramer (1822-1855). Dutch ophthalmologist.
9.
Handbuch der physiologischen Optik, edited by Nagel, 1909-11, vol. i,
p. 121.
10.
Ibid. vol. i, p. 122.
11.
The Refraction and Accommodation of the Eye and their Anomalies,
authorized translation by Culver, 1886, p. 151.
12.
Physiologic Optics, authorized translation by Weiland, 1904, p. 163.
Marius Hans Erik Tscherning (1854 - ) is a Danish
ophthalmologist who for twenty-five years was co-director and
director of the ophthalmological laboratory of the Sorbonne. Later he
became professor of ophthalmology in the University of Copenhagen.
13.
The Hygiene of the Eye in Schools, English translation edited by
Turnbull, 1886, p. 23. Hermann Cohn (1838-1906) was professor of
ophthalmology in the University of Breslau, and is known chiefly for
his contributions to ocular hygiene.
14.
Lessons in Elementary Physiology, sixth edition, 1872, p. 231.
15.
On the Anomalies of Accommodation and Refraction of the Eye, p. 13.
16.
Krankheiten des Auges, 1853-56, vol. iii, D. 219, et seq.
17.
Ueber die Ursachen und die Entstehung der Kurzsichtigkeit, 1876.
Vorwort.
18.
Handbuch der physiologischen Optik, vol. i, pp. 124 and 145.
19.
Ibid, vol. i. P. 144.
20.
Physiologic Optics, p. 166.
21.
Absence of the lens.
22.
On the Anomalies of Accommodation and Refraction of the Eye, p. 320.
23.
Archiv. f. Ophth., 1855, vol. ii, part 1, p. 187 et seq. Albrecht von
Graefe (1828-1870) was professor of ophthalmology in the University
of Berlin, and is ranked with Donders and Arlt as one of the greatest
ophthalmologists of the 19th century.
24.
Klin. Montasbl. f. Augenh., Erlangen, 1872, vol. x, p. 39, et seq.
25.
Archiv. f. Ophth., 1873, vol. xix, part 3, 107.
26.
Flint: Physiology of Man, 1875, vol. v, 110-111.
27.
Davis: Accommodation in the Lensless Eye, Reports of the Manhattan
Eye and Ear Hospital, Jan., 1895. The article gives a review of the
whole subject.
28.
An instrument for measuring the curvature of the cornea.
29.
Nov., 1893, p. 932.
30.
Inasmuch as the eye is inextensible, it cannot adapt itself for the
perception of objects situated at different distances by
increasing the length of its axis, but only by increasing the
refractive power of its lens. - De Schweinitz: Diseases of the
Eye, eighth
edition, 1916, pp. 35-36.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
IV
THE TRUTH ABOUT ACCOMMODATION AS DEMONSTRATED BY
EXPERIMENTS ON THE EYE MUSCLES OF FISH, CATS, DOGS, RABBITS AND OTHER
ANIMALS
THE
function of the muscles on the outside of the eyeball, apart from
that of turning the globe in its socket, has been a matter of much
dispute; but after the supposed demonstration by Helmholtz that
accommodation depends upon a change in the curvature of the lens, the
possibility of their being concerned in the adjustment of the
eye for vision at different distances, or in the production of errors
of refraction, was dismissed as no longer worthy of serious
consideration. "Before physiologists were acquainted with
the changes in the dioptic system,"(1) says Donders, "they
often attached importance to the external muscles in the production
of accommodation. Now that we know that accommodation depends on
a change of form in the lens this opinion seems scarcely to need
refutation." He states positively that "many instances
occur where the accommodation is wholly destroyed by paralysis,
without the external muscles being the least impeded in their
action," and also that "some cases are on record of
paralysis of all or nearly all of the muscles of the eye, and of
deficiency of the same, without diminution of the power of
accommodation."(2)
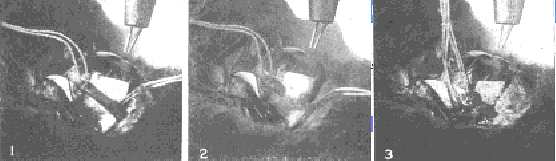
Fig.
13. Demonstration Upon the Eye of a Rabbit that the Inferior
Oblique Muscle is an Essential Factor in Accommodation
No.
1. - The inferior oblique muscle has been exposed and two sutures are
attached to it. Electrical stimulation of the eyeball produces
accommodation as demonstrated by simultaneous retinoscopy.
No.
2. - The muscle has been cut. Electrical stimulation produces no
accommodation.
No.
3. - The muscle has been sewed together. Electrical stimulation
produces normal accommodation.
Fig.
14. Demonstration Upon the Eye of a Carp That the Superior Oblique
Muscle Is Essential to Accommodation.
No.
1. - The superior oblique is lifted from the eyeball by two sutures,
and the retinoscope shows no error of refraction. No. 2. - Electrical
stimulation produces accommodation, as determined by the retinoscope.
No. 3. - The muscle has been cut. Stimulation of the eyeball with
electricity fails to produce accommodation. No. 4. - The divided
muscle has been reunited by tying the sutures. Accommodation follows
electrical stimulation as before.
If
Donders had not considered the question settled, he might have
inquired more carefully into these cases, and if he had, he might
have been less dogmatic in his statements; for, as has been pointed
out in the preceding chapter, there are plenty of indications that
the contrary is the case. In my own experiments upon the
extrinsic eye muscles of fish, rabbits, cats, dogs and other animals,
the demonstration seemed to be complete that in the eyes of
these animals accommodation depends wholly upon the action of
the extrinsic muscles and not at all upon the agency of the
lens. By the manipulation of these muscles I was able to produce or
prevent accommodation at will, to produce myopia, hypermetropia
and astigmatism, or to prevent these conditions.
Full
details of these experiments will be found in the "Bulletin
of the New York Zoological Society" for November, 1914, and in
the "New York Medical Journal" for May 8, 1915; and May 18,
1918; but for the benefit of those who have not
the time or inclination to read these papers, their contents
are summarized below.
There
are six muscles on the outside of the eyeball, four known as the
"recti" and two as the "obliques." The obliques
form an almost complete belt around the middle of the eyeball, and
are known, according to their position, as "superior" and
"inferior." The recti are attached to the sclerotic,
or outer coat of the eyeball, near the front, and pass directly over
the top, bottom and sides of the globe to the back of the orbit,
where they are attached to the bone round the edges of the hole
through which the optic nerve passes. According to their position,
they are known as the "superior," "inferior,"
"internal" and "external" recti.- The obliques
are the muscles of accommodation; the recti are concerned in the
production of hypermetropia and astigmatism.
In
some cases one of the obliques is absent or rudimentary, but when two
of these muscles were present and active, accommodation, as measured
by the objective test of retinoscopy, was always produced by
electrical stimulation either of the eyeball, or of the nerves of
accommodation near their origin in the brain. It was also
produced by any manipulation of the obliques whereby their pull
was increased. This was done by a tucking operation of one or both
muscles, or by an advancement of the point at which they are attached
to the sclerotic. When one or more of the recti had been cut, the
effect of operations increasing the pull of the obliques was
intensified.

Fig.
15. Demonstration Upon the Eye of a Rabbit That
the Production of
Refractive Errors Is Dependent Upon the Action of the External
Muscles. The String Is Fastened to the Insertion of the Superior
Oblique and Rectus Muscles --
No.
1. - Backward pull. Myopia is produced.
No.
2. - Forward pull. Hypermetropia is produced.
No.
3. - Upward pull in the plane of the iris. Mixed astigmatism is
produced.
After
one or both of the obliques had been cut across, or after they had
been paralyzed by the injection of atropine deep into the orbit,
accommodation could never be produced by electrical stimulation;
but after the effects of the atropine had passed away, or a divided
muscle had been sewed together, accommodation followed
electrical stimulation just as usual.
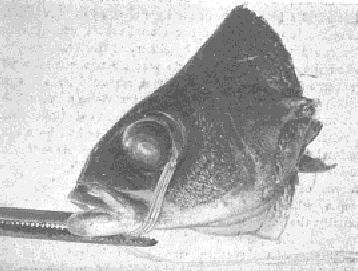
Fig.
16. Demonstration Upon the Eye of a Fish
That the Production of Myopic and Hypermetropic Refraction Is
Dependent Upon the Action of the Extrinsic Muscles.
Suture tied to the insertion of the superior rectus muscle.
By means of strong traction upon the suture the eyeball is turned in
its socket, and by tying the thread to a pair of fixation forceps
which grasp! the lower jaw, it is maintained in this position. A high
degree of mixed astigmatism is produced, as demonstrated by
simultaneous retinoscopy. When the superior oblique is divided
the myopic part of the astigmatism disappears, and when the
inferior rectus is cut the hypermetropic part disappears, and the eye
becomes normal - adjusted for distant vision - although the same
amount of traction is maintained. It is evident that these muscles
are essential factors in the production of myopia and hypermetropia.
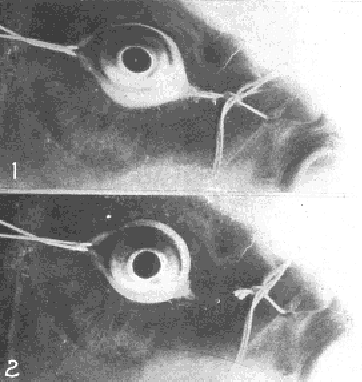
Fig.
17. -- No. 1. - Production of mixed astigmatism in the eye of
a carp by pulling strings attached to the conjunctiva in
opposite directions. Note the oval shape of the front of the eyeball.
No.
2. - With the cutting of the strings the eyeball returns to
its normal shape, and the refraction becomes normal.
Again
when one oblique muscle was absent, as was found to be the case
in a dogfish, a shark and a few perch, or rudimentary, as in all cats
observed, a few fish and an occasional rabbit, accommodation could
not be produced by electrical stimulation. But when the rudimentary
muscle was strengthened by advancement, or the absent one
was replaced by a suture which supplied the necessary
countertraction, accommodation could always be produced
by electrical stimulation.
After
one or both of the oblique muscles had been cut, and while two or
more of the recti were present and active,(3) electrical stimulation
of the eyeball, or of the nerves of accommodation, always
produced hypermetropia, while by the manipulation of one of the
recti, usually the inferior or the superior, so as to
strengthen its pull, the same result could be produced. The
paralyzing of the recti by atropine, or the cutting of one
or more of them, prevented the production of hypermetropic refraction
by electrical stimulation; but after the effects of the atropine
had passed away, or after a divided muscle had been sewed together,
hypermetropia was produced as usual by electrical stimulation.
It
should be emphasized that in order to paralyze either the recti
muscles, or the obliques, it was found necessary to inject the
atropine far back behind the eyeball with a hypodermic needle. This
drug is supposed to paralyze the accommodation when dropped into the
eyes of human beings or animals, but in all of my experiments
it was found that when used in this way it had very little effect
upon the power of the eye to change its focus.
Astigmatism
was usually produced in combination with myopic or hypermetropic
refraction. It was also produced by various manipulations of both the
oblique and recti muscles. Mixed astigmatism, which is a combination
of myopic with hypermetropic refraction, was always
produced by traction on the insertion of the superior or
inferior rectus in a direction parallel to the plane of the
iris, so long as both obliques were present and active; but if either
or both of the obliques had been cut, the myopic part of the
astigmatism disappeared.
Similarly
after the superior or the inferior rectus had been cut the
hypermetropic part of the astigmatism disappeared. Advancement of the
two obliques, with advancement of the superior and inferior recti,
always produced mixed astigmatism.
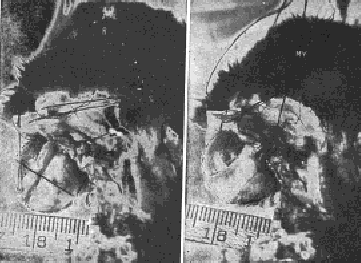
Fig.
18. Demonstration Upon the Eyeball of a Rabbit That the Obliques
Lengthen the Visual Axis in Myopia -- R, rest. The eyeball is of
normal length and emmetropic - that is, perfectly adjusted for
distant vision. My, myopia. The pull of the oblique muscles has been
strengthened by advancement and the retinoscope shows that myopia has
been produced. It can easily be noted that the eyeball is longer. It
was impossible to avoid some movement of the head between the taking
of the two pictures as a result of the manipulation of the strings,
but the rule shows that the focus of the camera was not appreciably
changed by such movements.
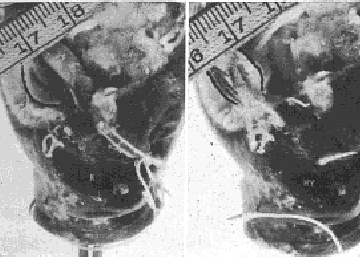
Fig.
19. Demonstration Upon the Eye of a Carp That the Recti Shorten
the Visual Axis in Hypermetropia -- R, rest. The eyeball is of
normal length and emmetropic. Hy, hypermetropia. The pull of the
external and internal recti has been strengthened by advancement, and
the retinoscope shows that hypermetropia has been produced. It
may easily be noted that the eyeball is shorter. The rule shows that
the focus of the camera was not appreciably changed between the
taking of the two pictures.
Eyes
from which the lens had been removed, or in which it had been pushed
out of the axis of vision, responded to electrical stimulation
precisely as did the normal eye, so long as the muscles were active;
but when they had been paralyzed by the injection of atropine deep
into the orbit, electrical stimulation had no effect on the
refraction.
In
one experiment the lens was removed from the right eye of a rabbit,
the refraction of each eye having first been tested by retinoscopy
and found to be normal. The wound was then allowed to heal.
Thereafter, for a period extending from one month to two years,
electrical stimulation always produced accommodation in the lensless
eye precisely to the same extent as in the eye which had a lens. The
same experiment with the same result was performed on a number of
other rabbits, on dogs and on fish. The obvious conclusion is that
the lens is not a factor in accommodation.
In
most text-books on physiology it is stated that accommodation is
controlled by the third cranial nerve, which supplies all the muscles
of the eyeball except the superior oblique and the external rectus;
but the fourth cranial nerve, which supplies only the superior
oblique, was found in these experiments to be just as much a nerve of
accommodation as the third.
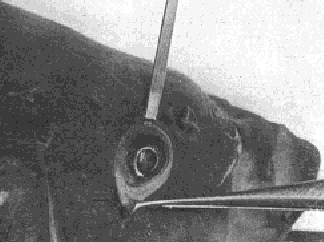
Fig.
20. Lens Pushed Out of the Axis of Vision
In
this experiment on the eye of a carp the lens was pushed out of the
axis of vision. Accommodation took place after this displacement just
as it did before. Note the point of the knife in the pupil in front
of the lens.

Fig.
21. Rabbit With Lens Removed -- The animal was exhibited at a
meeting of the Ophthalmological Section of the American Medical
Association, held in Atlantic City, and was examined by a number of
ophthalmologists present, all of whom testified that electrical
stimulation of the eyeball produced accommodation, or myopic
refraction, precisely as in the normal eye.
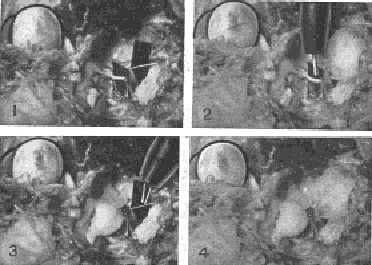
Fig.
22. Experiment Upon the Eye of a Cat Demonstrating That the
Fourth Nerve, Which Supplies Only the Superior Oblique Muscle, Is
Just as Much a Nerve of Accommodation As the Third, and That the
Superior Oblique Muscle Which It Supplies Is a Muscle of
Accommodation.
No.
1. - Both nerves have been exposed near their origin in the brain,
and a strip of black paper has been inserted beneath each to render
it visible. The fourth nerve is the smaller one The superior oblique
muscle has been advanced by a tucking operation, as this muscle
is always rudimentary in cats, and unless its pull is strengthened
accommodation cannot be produced in these animals. Stimulation of
either or both nerves by the faradic current produced accommodation.
No.
2. - When the fourth nerve was covered with cotton soaked in a normal
salt solution, the application of the faradic current to the
cotton produced accommodation. When the cotton was soaked in a one
per cent solution of atropine sulphate in a normal salt solution,
such application produced no accommodation, but stimulation of the
third nerve did produce it.
No.
3. When the third nerve was covered with cotton soaked in a normal
salt solution, the application of the faradic current to the
cotton produced accommodation. When the cotton was soaked with
atropine sulphate in a normal salt solution, such application
produced no accommodation, but the stimulation of the fourth
nerve did produce it.
No.
4. - When both nerves were covered with cotton soaked in atropine
sulphate in a normal salt solution, the application of electricity to
the cotton produced no accommodation. When the parts had been washed
with a warm salt solution electrical stimulation of either nerve
always produced accommodation. The nerves were alternately covered
with the atropine-soaked cotton and then washed with the warm saline
solution for an hour the electricity being applied in each condition
with invariably the same result. Accommodation could never be
produced by electrical stimulation when the nerves were paralyzed
with the atropine, but always resulted from the stimulation of either
or both when they had been washed with the salt solution. The
experiment was performed with the same results on many rabbits and
dogs.
When
either the third or the fourth nerve was stimulated with
electricity near its point of origin in the brain accommodation
always resulted in the normal eye. When the origin of either nerve
was covered with a small wad of cotton soaked in a two per cent
solution of atropine sulphate in a normal salt solution,
stimulation of that nerve produced no accommodation, while
stimulation of the unparalyzed nerve did produce it. When the
origin of both nerves was covered with cotton soaked in atropine,
accommodation could not be produced by electrical stimulation of
either or both. When the cotton was removed and the nerves
washed with normal salt solution, electrical stimulation of
either or both produced accommodation just as before the
atropine had been applied. This experiment, which was performed
repeatedly for more than an hour by alternately applying and removing
the atropine, not only demonstrated clearly what had not
been known before, namely, that the fourth nerve is a nerve of
accommodation, but also demonstrated that the superior oblique
muscle which is supplied by it is an important factor in
accommodation. It was further found that when the action of the
oblique muscles was prevented by dividing them, the stimulation of
the third nerve produced, not accommodation, but hypermetropia.
In
all the experiments all sources of error are believed to have been
eliminated. They were all repeated many times and always with the
same result. They seemed, therefore, to leave no room for doubt
that neither the lens nor any muscle inside the eyeball has anything
to do with accommodation, but that the process whereby the eye
adjusts itself for vision at different distances
is entirely controlled
by the action of the muscles on the outside of the globe.
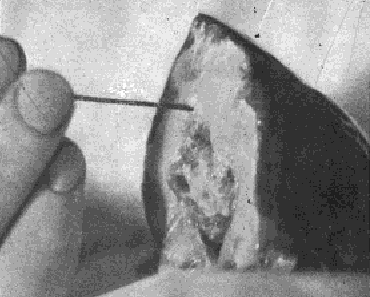
Fig.
23. Pithing a Fish Preparatory to Operating Upon Its Eyes --
The object of this operation is to secure greater relaxation of the
muscles of the eyes and head, which would work for hours, without
external stimulus, if the brain cells were not destroyed by the
probe.
CITATIONS
1.
The refractive system.
2.
On the Anomalies of Accommodation and Refraction of the Eye, p. 22.
3.
In many animals, notably in rabbits, the internal and external recti
are either absent or rudimentary, so that. practically, in such
cases, there are only two recti, just as there are only two
obliques. In others, as in many fish, the internal rectus is
negligible.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
V
THE TRUTH ABOUT ACCOMMODATION AS DEMONSTRATED BY A STUDY OF
IMAGES REFLECTED FROM THE LENS, CORNEA, IRIS AND SCLERA
As
the conclusions to which the experiments described in the preceding
chapter pointed were diametrically opposed to those reached by
Helmholtz in his study of the images reflected from the front of the
lens, I determined to repeat the experiments of the German
investigator and find out, if possible, why his results were so
different from my own. I devoted four years to this work, and was
able to demonstrate that Helmholtz had erred through a defective
technique, the image obtained by his method being so variable and
uncertain that it lends itself to the support of almost any theory.
I
worked for a year or more with the technique of Helmholtz, but was
unable to obtain an image from the front of the lens which was
sufficiently clear or distinct to be measured or photographed.
With a naked candle as the source of light a clear and distinct image
could be obtained on the cornea; on the back of the lens it was quite
clear; but on the front of the lens it was very imperfect. Not
only was it blurred, just as Helmholtz stated, but without any
ascertainable cause it varied greatly in size and intensity. At times
no reflection could be obtained at all, regardless of the angle of
the light to the eye of the subject, or of the eye of the observer to
that of the subject. With a diaphragm I got a clearer and more
constant image, but it still was not sufficiently reliable to be
measured.
To
Helmholtz the indistinct image of a naked flame seemed to show an
appreciable change, while the images obtained by the aid of the
diaphragm showed
it
more clearly; but I was unable, either with a diaphragm or
without it, to obtain images which I considered sufficiently distinct
to be reliable.
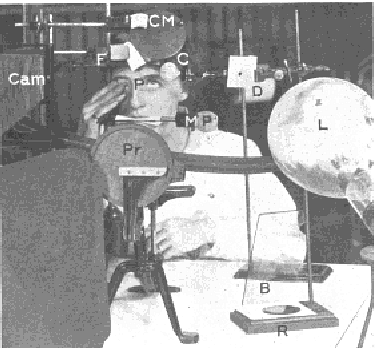
Fig.
24. Arrangements for Photographing Images Reflected From the
Eyeball -- CM, concave mirror in which the subject may
observe the images reflected from various parts of her eye- C,
condenser; D, diaphragm; L, 1000-watt lamp; F, forehead rest; MP, bar
which the subject grasps with her teeth for the purpose of holding
her head steady- P, plane mirror upon which is pasted a letter of
diamond type and in which is reflected a Snellen test card twenty
feet behind the subject (the mirror is just above the letter P); CAM,
camera; Pr, perimeter used to measure the angle of the light to
the eye; R, plane mirror reflecting light from the 1000-watt
lamp upon the eye, which otherwise would be in total darkness except
for the part from which the highly condensed image of the filament is
reflected; B, blue glass screen used to modify the light reflected
from the mirror R. When the subject read the bottom line of the
Snellen test card reflected in the mirror P her eye was at rest, and
when she saw the letter of diamond type distinctly it was
accommodated ten diopters, as demonstrated by the retinoscope.
With
a thirty-watt lamp, a fifty-watt lamp, a 250-watt lamp and a
1000-watt lamp, there was no
improvement.
The
light of the sun reflected from the front of the lens produced an
image just as cloudy and uncertain as the reflections from other
sources of illumination, and just as variable in shape,
intensity and size.
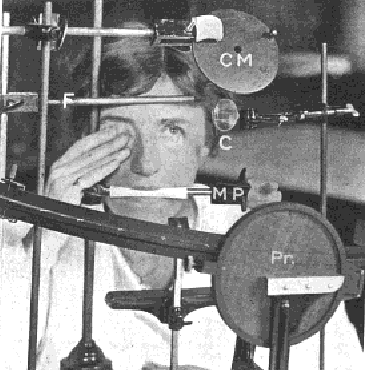
Fig.
25. Arrangements for Holding the Head of the Subject Steady While
Images Were Being Photographed. CM, concave mirror; F,
forehead rest; C, condenser, MP, mouthpiece; Pr, perimeter.
Men
who had been teaching and demonstrating Helmholtz's theory
repeated his experiments for my benefit; but the images which they
obtained on the front of the lens did not seem to me any better than
my own. After studying these images almost daily for more than a year
I was unable to make any reliable observation regarding the effect of
accommodation upon them. In fact, it seemed that an infinite number
of appearances might be obtained on the front of the lens when a
candle was used as the source of illumination. At times the image
became smaller during accommodation and seemed to sustain the theory
of Helmholtz; but just as frequently it became larger. At other times
it was impossible to tell what it did.
To
sum it all up, I was convinced that the anterior surface of the lens
was a very poor reflector of light, and that no reliable images could
be obtained from it by the means described.
After
a year or more of failure I began to work at an aquarium on the eyes
of fish. It was a long story of failure. Finally I became able, with
the aid of a strong light
- 1000 watts - a diaphragm with
a small opening and a condenser, to obtain, after some
difficulty, a clear and distinct image from the cornea of fish.
This image was sufficiently distinct to be measured, and
after many months a satisfactory photograph was obtained. Then
the work was resumed on the eyes of human beings. The strong light,
combined with the diaphragm and condenser, the use of which was
suggested by their use to improve the illumination of a glass
slide under the microscope, proved to be a decided improvement over
the method of Helmholtz, and by means of this technique an image
was at last obtained on the front of the lens which was sufficiently
clear and distinct to be photographed. This was the first time, so
far as published records show, that an image of any kind was ever
photographed from the front of the lens. Professional photographers
whom I consulted with a view to securing their assistance
assured me that the thing could not be done, and declined to attempt
it. I was therefore obliged to learn photography, of which I had
previously known nothing, myself, and I then found that so far as the
image obtained by the method of Helmholtz is concerned the
professionals were right.
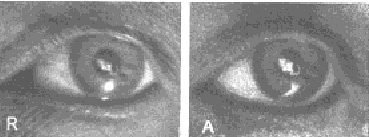
Fig.
26. Image of Electric Filament on the Front of the Lens -- R,
rest; A, accommodation. Under the magnifying glass no change can be
observed in the size of the two images. The image at the right looks
larger only because it is more distinct. To support the theory of
Helmholtz it ought to be the smaller. The comet's tail at the left of
the two images is an accidental reflection from the cornea. The spot
of light beneath is a reflection from the light used to illuminate
the eye while the photographs were being taken. It took two years to
get these pictures.
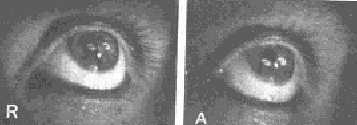
Fig.
27. Images of the Electric Filament Reflected Simultaneously From the
Cornea and Lens -- R, rest; A, accommodation. The size of the
images in both pictures is the same. The corneal image is so small
that it has not been noticeably altered by the slight change that
takes place in the cornea during accommodation. In A both images have
changed their position and the end of the reflection from the lens
has been cut off by the iris, but its width remains the same. The
white spot between the two images of the filament is a reflection
from the lamp used to illuminate the eye. Note that in A more of the
sclera is visible, owing to the elongation of the eyeball during
accommodation.
Fig.
28. Image of Electric Filament Upon the Cornea --
R,
rest; A, accommodation. The image is smaller in A, but the change is
so slight as to be scarcely noticeable, showing that the
alteration in the shape of the cornea during accommodation is very
slight. For this reason the ophthalmometer, with its small
image, has been thought to demonstrate that the cornea did
not change during accommodation.
Fig.
29. Image of Electric Filament on the Front of the Sclera --
R, rest; A, accommodation. During accommodation the front
of the sclera becomes more convex, because the eyeball has elongated,
just as a camera is elongated when it is focussed upon a near object.
The spot of light on the cornea is an accidental reflection.
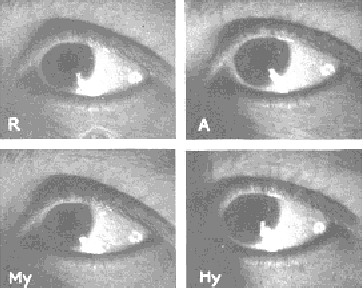
Fig.
30. Images on the Side of the Sclera -- R, rest; A,
accommodation. The image in A is the larger, indicating a flattening
of the side of the sclera as the eyeball elongates. My, Myopia.
The eye is straining to see at the distance and the image is
larger, indicating that the eyeball has elongated, resulting in a
flattening of the side of the sclera. Hy, Hypermetropia. The eye
is straining to see at two inches. The image is the smallest of
the series, indicating that the eyeball has become shorter than
in any of the other pictures, and the side of the sclera more
convex. The two lower pictures confirm the author's previous
observations that farsight is produced when the eye strains to see
near objects and nearsight when it strains to see distant objects.

Fig.
31. Multiple Images Upon the Front of the Lens -- This
picture illustrates one of the difficulties that had to be overcome
in photographing images reflected from various parts of the
eyeball. Unless the light was adjusted at precisely the right angle
the filament was multiplied by reflection from the sides of the
globe. Usually the image was doubled, sometimes it was tripled, as
shown in the picture, and sometimes it was quadrupled. Often days of
labor were required to eliminate these reflections, and for reasons
that were not definitely determined the same adjustment did not
always give the same results. Sometimes all would go well for
days, and then, without any apparent reason, the multiple images
would return.
Fig.
32. Reflection of the Electric Filament From the Iris
This
picture is shown to illustrate the fact that it is possible to get a
reflection from any reflecting surface of the eyeball without
reflections from the other parts, although these may be exposed. This
is done by changing the angle of the light to the eye. In No. 1
observations of the eye at the time the picture was taken
demonstrated that the image was from the iris, not from the cornea,
and the fact is also apparent in the picture. (Compare the image with
the corneal reflection in Fig. 28.) In No. 2, where the image
overlaps the margin of the pupil, the fact that the reflection is
from the iris is manifest from the circumstance that only part of the
filament is seen. If it were from the cornea, the whole of it would
be reflected. Note in this picture that there is no reflection from
the lens. The images on the iris did not change their size or shape
during accommodation, demonstrating again that the lens, upon which
the iris rests, does not change its shape when the eye adjusts itself
for near vision.
The
experiments were continued until, after almost four years of
constant labor, I obtained satisfactory pictures before and after
accommodation and during the production of myopia and
hypermetropia, not only of images on the front of the lens, but of
reflections from the iris, cornea,
the
front of the sclera (white of the
eye) and the side of the sclera. I also became able to obtain
images on any surface at will
without reflections from the other parts. Before these results were
obtained, however, many difficulties had still to be overcome.
Complicating
reflections were a perpetual source of trouble. Reflections from
surrounding objects were-easily prevented; but those from the sides
of the globe of the electric light were difficult to deal with, and
it was useless to try to obtain images on the front of the lens
until they had been eliminated, or reduced to a minimum, by a proper
adjustment of the light. The same apparent adjustment did
not, however, always give similar results. Sometimes there
would be no reflections for days; then would come a day when,
with the light apparently at the same angle, they would
reappear.
With
some adjustments of the light multiple images were seen
reflected from the front of the lens. Sometimes these images
were arranged in a horizontal line, sometimes in a vertical
one and sometimes at angles of different degrees, while
their distance from each other also varied.
Usually
there were three of them; sometimes there were more; and sometimes
there were only two. Occasionally they were all of the same size, but
usually they varied, there being apparently no limit to their
possibilities of change in this and other respects. Some were
photographed, indicating that they were real reflections.
Changes in the distance of the diaphragm from the light and from the
condenser, and alterations in the size and shape of its
opening, appeared to make no difference. Different adjustments
of the condenser were equally without effect. Changes in
the angle at which the light was adjusted sometimes lessened the
number of images and sometimes increased them, until at last an
angle was found at which but one image was seen. The images appear,
in fact, to have been caused by reflections from the globe of the
electric light.
Even
after the light had been so adjusted as to eliminate reflections it
was often difficult, or impossible, to get a clear and
distinct image of the electric filament upon the front of the lens.
One
could rearrange the condenser and the diaphragm and change the axis
of fixation, and still the image would be clouded or obscured
and its outline distorted. The cause of the difficulty appeared to be
that the light was not adjusted at the best angle for the purpose and
it was not always possible to determine the exact axis at which a
clear, distinct image would be produced. As in the case of the
reflections from the sides of the globe, it seemed to vary
without a known cause. This was true, however: that there were angles
of the axis of the globe which gave better images than others, and
that what these angles were could not be determined with exactness. I
have labored with the light for two or three hours without finding
the right angle. At other times the axis would remain unchanged for
days, giving always a clear, distinct image.
The
results of these experiments confirmed the conclusions drawn from the
previous ones, namely, that accommodation is due to a lengthening
of the eyeball, and not to a change in the curvature of the lens.
They also confirmed, in a striking manner, my earlier
conclusions as to the conditions under which myopia and
hypermetropia are produced.(1)
The
images photographed from the front of the lens did not show any
change in size or form during accommodation. The image on the back of
the lens also remained unchanged, as observed through the telescope
of the ophthalmometer; but as there is no dispute about its
behavior during accommodation, it was not photographed. Images
photographed from the iris before and during accommodation were also
the same in size and form, as was to be expected from the
character of the lens images. If the lens changed during
accommodation, the iris, which rests upon it, would change also.
The
images photographed from the cornea and from the front and side of
the sclera showed, however, a series of four well-marked changes,
according to whether the vision was normal or accompanied by a
strain. During accommodation the images from the cornea were smaller
than when the eye was at rest, indicating elongation of the eyeball
and a consequent increase in the convexity of the cornea. But when an
unsuccessful effort was made to see at the near-point, the
image became larger, indicating that the cornea had become less
convex, a condition which one would expect when the optic axis was
shortened, as in hypermetropia. When a strain was made to see at a
distance the image was smaller than when the eye was at rest, again
indicating elongation of the eyeball and increased convexity of
the cornea.
The
images photographed from the front of the sclera showed the same
series of changes as the corneal images, but those obtained from the
side of the sclera were found to have changed in exactly the opposite
manner, being larger where the former were smaller and vice versa, a
difference which one would naturally expect from the fact that
when the front of the sclera becomes more convex the sides must
become flatter.
When
an effort was made to see at a distance the image reflected from the
side of the sclera was larger than the image obtained when the eye
was at rest, indicating that this part of the sclera had become less
convex or flatter, because of elongation of the eyeball. The image
obtained during normal accommodation was also larger than when the
eye was at rest, indicating again a flattening of the side of
the sclera. The image obtained, however, when an effort was made
to see near was much smaller than any of the other images, indicating
that the sclera had become more convex at the side, a condition which
one would expect when the eyeball was shortened, as in
hypermetropia.
The
most pronounced of the changes were noted in the images reflected
from the front of the sclera. Those on the side of the sclera were
less marked, and, owing to the difficulty of photographing a
white image on a white background, could not always be readily seen
on the photographs. They were always plainly apparent, however,
to the observer, and still more so to the subject, who regarded them
in a concave mirror.
The
alterations in the size of the corneal image were so slight that they
did not show at all in the photographs, except when the image was
large, a fact which explains why the ophthalmometer, with its small
image, has been thought to show that the cornea did not change during
accommodation. They were always apparent, however, to the
subject and observer.
The
corneal image was one of the easiest of the series to produce and the
experiment is one which almost anyone can repeat, the only apparatus
required being a fifty-candlepower lamp - an ordinary electric
globe - and a concave mirror fastened to a rod which moves back
and forth in a groove so that the distance of the mirror from the eye
can be altered at will. A plane mirror might also be used; but the
concave glass is better, because it magnifies the image. The
mirror should be so arranged that it reflects the image of the
electric filament on the cornea, and so that the eye of the
subject can see this reflection by looking straight ahead. The
image in the mirror is used as the point of fixation, and the
distance at which the eye focuses is altered by altering the distance
of the mirror from the eye. The light can be placed within an inch or
two of the eye, as the heat is not great enough to interfere
with the experiment. The closer it is the larger the image, and
according to whether it is adjusted vertically, horizontally, or at
an angle, the clearness of the reflection may vary. A blue
glass screen can be used, if desired, to lessen the discomfort of the
light. If the left eye is used by the subject - and in all the
experiments it was found to be the more convenient for the purpose -
the source of light should be placed to the left of
that eye and as much as possible to the front of it, at an angle of
about forty-five degrees. For absolute accuracy the light and the
head of the subject should be held immovable, but for demonstration
this is not essential. Simply holding the bulb in his hand the
subject can demonstrate that the image changes according to whether
the eye is at rest, accommodating normally for near vision, or
straining to see at a near or a distant point. In the original
report were described possible sources of error and the means
taken to eliminate them.
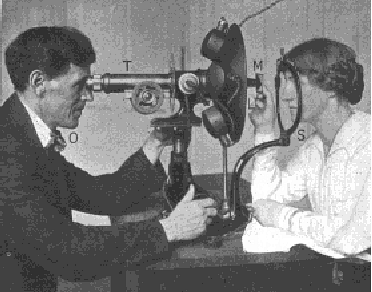
Fig.
33. Demonstrating That the Back of the Lens Does Not Change During
Accommodation. -- The filament of an electric light (L) is
shining into the eye of the subject (S), and the reflection on the
back of the lens can be seen by the observer (O) in the telescope
(T). The subject holds in her hand, at a distance of four inches, a
mirror on which is pasted a small letter, and in which is reflected a
Snellen test card hung above and behind her head at a distance of
twenty feet. The retinoscope reveals that when she looks at the
reflection of the test card and reads the bottom line the eye is at
rest, and that when she looks at the letter pasted on the mirror it
accommodates. The image on the lens does not change during these
changes of focus. The telescope is the telescope of the
ophthalmometer, the prisms having been removed. As there is no
dispute about the behavior of the back of the lens during
accommodation this image was not photographed.
CITATIONS
1.
Bates: The Cause of Myopia, N. Y. Med. Jour., March 16, 1912.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
VI
THE TRUTH ABOUT ACCOMMODATION AS DEMONSTRATED BY CLINICAL
OBSERVATIONS
The
testimony of the experiments described in the preceding chapters to
the effect that the lens is not a factor in accommodation is
confirmed by numerous observations on the eyes of adults and
children, with normal vision, errors of refraction, or
amblyopia, and on the eyes of adults after the removal of the lens
for cataract.
It
has already been pointed out that the instillation of atropine
into the eye is supposed to prevent accommodation by paralyzing the
muscle credited with controlling the shape of the lens. That it
has this effect is stated in every text-book on the subject,(1) and
the drug is daily used in the fitting of glasses for the purpose
of eliminating the supposed influence of the lens upon
refractive states.
In
about nine cases out of ten the conditions resulting from the
instillation of atropine into the eye fit the theory upon which its
use is based; but in the tenth case they do not, and every
ophthalmologist of any experience has noted some of these tenth
cases. Many of them are reported in the literature, and many of them
have come under my own observation. According to the theory, atropine
ought to bring out latent hypermetropia in eyes either apparently
normal, or manifestly hypermetropic, provided, of course,
the patient is of the age
during which the lens is supposed to retain its elasticity. The fact
is that it sometimes produces myopia, or changes
hypermetropia
into myopia, and that it will produce both myopia and hypermetropia
in persons over seventy years of age, when the lens is supposed to be
as hard as a stone, as well as in cases in which the lens is hard
with incipient cataract.
Patients
with eyes apparently normal will, after the use of atropine, develop
hypermetropic astigmatism, or myopic astigmatism, or compound
myopic astigmatism, or mixed astigmatism.(2) In other cases the
drug will not interfere with the accommodation, or alter the
refraction in any way. Furthermore, when the vision has been lowered
by atropine the subjects have often become able, simply by
resting their eyes, to read diamond type at six inches. Yet atropine
is supposed to rest the eyes by affording relief to an
overworked muscle.
In
the treatment of squint and amblyopia I have often Used atropine in
the better eye for more than a year, in order to encourage the use of
the amblyopic eye; and at the end of this time, while still under the
influence of atropine, such eyes have become able in a few hours, or
less, to read diamond type at six inches (see Chapter XXII). The
following are examples of many similar cases that might be cited:
A
boy of ten had hypermetropia in both eyes, that of the left or better
eye amounting to three diopters. When atropine was instilled
into this eye the hypermetropia was increased to four and a half
diopters, and the vision lowered to 20/200. With a convex glass
of four and a half diopters the patient obtained normal vision for
the distance, and with the addition of another convex glass of
four diopters he was able to read diamond type at ten inches
(best). The atropine was used for a year, the pupil being dilated
continually to the maximum.
Meantime
the right eye was being treated by methods to be described later.
Usually in such cases the eye which is not being specifically treated
improves to some extent with the others, but in this case it did not.
At the end of the year the vision of the right eye had become normal;
but that of the left eye remained precisely what it was at the
beginning, being still 20/200 without glasses for the distance,
while reading without glasses was impossible and the degree of the
hypermetropia had not changed. Still under the influence of the
atropine and still with the pupil dilated to the maximum, this
eye was now treated separately; and in half an hour its vision had
become normal both for the distance and the nearpoint, diamond type
being read at six inches, all without glasses. According to the
accepted theories, the ciliary muscle of this eye must not only have
been completely paralyzed at the time, but must have been in a
state of complete paralysis for a year. Yet the eye not only
overcame four and a half diopters of hypermetropia, but added six
diopters of accommodation, making a total of ten and a half. It
remains for those who adhere to the accepted theories to say how such
facts can be reconciled with them.
Equally,
if not more remarkable, was the case of a little girl of six who had
two and a half diopters of hypermetropia in her right or better
eye, and six in the other, with one diopter of astigmatism. With the
better eye under the influence of atropine and the pupil dilated
to the maximum, both eyes were treated together for more than a year,
and at the end of that time, the right being still under the
influence of the atropine, both became able to read diamond type
at six inches, the right doing it better, if anything, than the
left. Thus, in spite of the atropine, the right eye not only
overcame two and a half diopters of hypermetropia, but
added six diopters of accommodation, making a total of eight and a
half. In order to eliminate all possibility of latent hypermetropia
in the left eye - which in the beginning had six diopters - the
atropine was now used in this eye and discontinued in the other,
the eye education being continued as before. Under the influence
of the drug there was a slight return of the hypermetropia; but the
vision quickly became normal again, and although the atropine was
used daily for more than a year, the pupil being continually
dilated to the maximum, it remained so, diamond type being read
at six inches without glasses during the whole period. It is
difficult for me to conceive how the ciliary muscle could have
had anything to do with the ability of this patient to accommodate
after atropine had been used in each eye separately for a year or
more at a time.
According
to the current theory, atropine paralyzes the ciliary muscle and
thus, by preventing a change of curvature in the lens, prevents
accommodation. When accommodation occurs, therefore, after
the prolonged use of atropine, it is evident that it must be due to
some factor or factors other than the lens and the ciliary muscle.
The evidence of such cases against the accepted theories is, in fact,
overwhelming; and according to these theories the other factors
cited in this chapter are equally inexplicable. All of these facts,
however, are in entire accord with the results of my experiments
on the eye muscles of animals and my observations regarding the
behavior of images reflected from various parts of the eyeball. They
strikingly confirm, too, the testimony of the experiments with
atropine, which showed that the accommodation could not be paralyzed
completely and permanently unless the atropine was injected deep into
the orbit, so as to reach the oblique muscles, the real muscles of
accommodation, while hypermetropia could not be prevented when
the eyeball was stimulated with electricity without a similar
use of atropine, resulting in the paralysis of the recti
muscles.
As
has already been noted, the fact that after the removal of the lens
for cataract the eye often appears to accommodate just as well
as it did before is well known. Many of these cases have come under
my own observation. Such patients have not only read diamond type
with only their distance glasses on, at thirteen and ten inches and
at a less distance, but one man was able to read without any glass at
all. In all these cases the retinoscope demonstrated that the
apparent act of accommodation was real, being accomplished, not by
the "interpretation of circles of diffusion," or by any of
the other methods by which this inconvenient phenomenon is
commonly explained, but by an accurate adjustment of the focus to the
distances concerned.
The
cure of presbyopia (see Chapter XX) must also be added to the
clinical testimony against the accepted theory of accommodation. On
the theory that the lens is a factor in accommodation such cures
would be manifestly impossible. The fact that rest of the eyes
improves the sight in presbyopia has been noted by others, and has
been attributed to the supposed fact that the rested ciliary muscle
is able for a brief period to influence the hardened lens; but while
it is conceivable that this might happen in the early stages of
the condition and for a few moments, it is not conceivable that
permanent relief should be obtained by this means, or that
lenses which are, as the saying goes, as "hard as a stone,"
should be influenced, even momentarily.
A
truth is strengthened by an accumulation of facts. A working
hypothesis is proved not to be a truth if a single fact is not in
harmony with it. The accepted theories of accommodation and of the
cause of errors of refraction require that a multitude of facts shall
be explained away. During more than thirty years of clinical
experience, I have not observed a single fact that was not in harmony
with the belief that the lens and the ciliary muscle have nothing to
do with accommodation and that the changes in the shape of
the eyeball upon which errors of refraction depend are not permanent.
My clinical observations have of themselves been sufficient to
demonstrate this fact. They have also been sufficient to show how
errors of refraction can be produced at will, and how they may be
cured, temporarily in a few minutes, and permanently by continued
treatment.
CITATIONS
1.
Certain substances have the power of producing dilation of the pupil
(mydriasis) and hence are termed mydriatics. At the same time they
act upon the ciliary body diminishing and when applied in sufficient
strength completely paralyzing the power of accommodation thus
rendering the eye for some time unalterably focused for the farthest
point - Herman Snellen Jr.: Mydriatics and Myotics System of Diseases
of the Eye, edited by Norris and Oliver, 1897-1900, vol. ii, p. 30.
2.
In simple hypermetropic astigmatism one principal meridian is normal
and the other, at right angles to it, is flatter. In simple myopic
astigmatism the contrary is the case.; one principle meridian is
normal and the other, at right angles to it more convex. In mixed
astigmatism one principal meridian is too flat the other too convex.
In compound hypermetropic astigmatism both principal meridians are
flatter than normal one more so than the other. In compound myopic
astigmatism both are more convex than normal, one more so than the
other.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
VII
THE VARIABILITY OF THE REFRACTION OF THE EYE
The
theory that errors of refraction are due to permanent deformations of
the eyeball leads naturally to the conclusion, not only that errors
of refraction are permanent states, but that normal refraction is
also a continuous condition. As this theory is almost universally
accepted as a fact, therefore, it is not surprising to find that the
normal eye is generally regarded as a perfect machine which is
always in good working order. No matter whether the object
regarded is strange or familiar, whether the light is good or
imperfect, whether the surroundings are pleasant or disagreeable,
even under conditions of nerve strain or bodily disease, the
normal eye is expected to have normal refraction and normal
sight all the time. It is true that the facts do not harmonize with
this view, but they are conveniently attributed to the perversity
of the ciliary muscle, or if that explanation will not work, ignored
altogether.
When
we understand, however, how the shape of the eyeball is controlled by
the external muscles, and how it responds instantaneously to their
action, it is easy to see that no refractive state, whether it is
normal or abnormal, can be permanent. This conclusion is
confirmed by the retinoscope, and I had observed the facts long
before the experiments described in the preceding chapters had
offered a satisfactory explanation for it. During thirty years
devoted to the study of refraction, I have found few people
who could maintain perfect sight for more than a few
minutes at a time, even under the most favorable conditions; and
often I have seen the refraction change half a dozen times or more in
a second, the variations ranging all the way from twenty diopters of
myopia to normal. Similarly I have found no eyes with continuous or
unchanging errors of refraction, all persons with errors of
refraction having, at frequent intervals during the day and night,
moments of normal vision, when their myopia, hypermetropia, or
astigmatism, wholly disappears. The form of the error also
changes, myopia even changing into hypermetropia, and one form of
astigmatism into another.
Of
twenty thousand school children examined in one year, more than half
had normal eyes, with sight which was perfect at times; but not one
of them had perfect sight in each eye at all times of the day. Their
sight might be good in the morning and imperfect in the afternoon, or
imperfect in the morning and perfect in the afternoon. Many children
could read one Snellen test card: with perfect sight, while unable to
see a different one perfectly. Many could also read some letters of
the alphabet perfectly, while unable to distinguish other letters of
the same size under similar conditions. The degree of this
imperfect sight varied within wide limits, from one-third to
one-tenth, or less. Its duration was also variable. Under some
conditions it might continue for only a few minutes, or less; under
others it might prevent the subject from seeing the blackboard for
days, weeks, or even longer. Frequently all the pupils in a classroom
were affected to this extent.
Among
babies a similar condition was noted. Most investigators have found
babies hypermetropic. A few have found them myopic. My own
observations indicate that the refraction of infants is continually
changing. One child was examined under atropine on four successive
days, beginning two hours after birth. A three per cent solution of
atropine was instilled into both eyes, the pupil was dilated to the
maximum, and other physiological symptoms of the use of atropine
were noted. The first examination showed a condition of mixed
astigmatism. On the second day there was compound hypermetropic
astigmatism, and on the third compound myopic astigmatism.
On the fourth one eye was normal and the other showed simple myopia.
Similar variations were noted in many other cases.
What
is true of children and infants is equally true of adults of all
ages. Persons over seventy years of age have suffered losses of
vision of variable degree and intensity, and in such cases the
retinoscope always indicated an error of refraction. A man eighty
years old, with normal eyes and ordinarily normal sight, had periods
of imperfect sight which would last from a few minutes to half an
hour or longer. Retinoscopy at such times always indicated myopia of
four diopters or more.
During
sleep the refractive condition of the eye is rarely, if ever, normal.
Persons whose refraction is normal when they are awake will produce
myopia, hypermetropia and astigmatism when they are asleep, or, if
they have errors of refraction when they are awake, they will be
increased during sleep. This is why people waken in the morning
with eyes more tired than at any other time, or even with severe
headaches.
When
the subject is under ether or chloroform, or unconscious from
any other cause, errors of refraction are also produced or increased.
When
the eye regards an unfamiliar object an error of refraction is always
produced. Hence the proverbial fatigue caused by viewing pictures,
or other objects, in a museum. Children with normal eyes who can read
perfectly small letters a quarter of an inch high at ten feet always
have trouble in reading strange writing on the blackboard, although
the letters may be two inches high. A strange map, or any map, has
the same effect. I have never seen a child, or a teacher, who could
look at a map at the distance without becoming nearsighted.
German type has been accused of being responsible for much of the
poor sight once supposed to be peculiarly a German malady; but if a
German child attempts to read Roman print, it will at once become
temporarily hypermetropic. German print, or Greek or Chinese
characters, will have the same effect on a child, or other person,
accustomed to Roman letters.
Cohn
repudiated the idea that German lettering was trying to the eyes.(1)
On the contrary, he always found it "pleasant, after a long
reading of the monotonous Roman print, to return 'to our beloved
German."' Because the German characters were more familiar to
him than any others he found them restful to his eyes. "Use,"
as he truly observed, "has much to do with the matter."
Children learning to read, write, draw, or sew, always suffer from
defective vision, because of the unfamiliarity of the lines or
objects with which they are working.
A
sudden exposure to strong light, or rapid or sudden changes of light,
are likely to produce imperfect sight in the normal eye, continuing
in some cases for weeks and months (see Chapter XVII).
Noise
is also a frequent cause of defective vision in the normal eye. All
persons see imperfectly when they hear an unexpected loud noise.
Familiar sounds do not lower the vision, but unfamiliar ones always
do. Country children from quiet schools may suffer from defective
vision for a long time after moving to a noisy city. In school they
cannot do well with their work, because their sight is impaired. It
is, of course, a gross injustice for teachers and others to scold,
punish, or humiliate such children.
Under
conditions of mental or physical discomfort, such as pain,
cough, fever, discomfort from heat or cold, depression, anger, or
anxiety, errors of refraction are always produced in the normal
eye, or increased in the eye in which they already exist.
The
variability of the refraction of the eye is responsible for many
otherwise unaccountable accidents. When people are struck down
in the street by automobiles, or trolley cars, it is often due to the
fact that they were' suffering from temporary loss of sight.
Collisions on railroads or at sea, disasters in military operations,
aviation accidents, etc., often occur because some responsible person
suffered temporary loss of sight.
To
this cause must also be ascribed, in a large degree, the confusion
which every student of the subject has noted in the statistics which
have been collected regarding the occurrence of errors of refraction.
So far as I am aware it has never been taken into account by any
investigator of the subject; yet the result in any such
investigation must be largely determined by the conditions under
which it is made. It is possible to take the best eyes in the world
and test them so that the subject will not be able to get into the
Army. Again, the test may be so
made
that eyes which are apparently much below normal at the beginning,
may in the few minutes required for the test, acquire normal vision
and become able to read the test card perfectly.
CITATIONS
1
Eyes and School-Books Pop. Sci. Monthly, May, 1881, translated from
Deutsche Rundschau.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
VIII
WHAT GLASSES DO TO US
The
Florentines were doubtless mistaken in supposing that their
fellow citizen (see page v) was the inventor of the lenses now so
commonly worn to correct errors of refraction. There has been much
discussion as to the origin of these devices, but they are generally
believed to have been known at a period much earlier than that of
Salvino degli Armati.
The
Romans at least must have known something of the art of
supplementing the powers of the eye, for Pliny tells us that
Nero used to watch the games in the Colosseum through a concave gem
set in a ring for that purpose. If, however, his contemporaries
believed that Salvino of the Armati was the first to produce
these aids to vision, they might well pray for the pardon of his
sins; for while it is true that eyeglasses have brought to some
people improved vision and relief from pain and discomfort, they have
been to others simply an added torture, they always do more or less
harm, and at their best they never improve the vision to normal.
That
glasses cannot improve the sight to normal can be very simply
demonstrated by looking at any color through a strong convex or
concave glass. It will be noted that the color is always less intense
than when seen with the naked eye; and since the perception of form
depends upon the perception of color, it follows that both color and
form must be less distinctly seen with glasses than without them.
Even plane glass lowers the vision both for color and form, as
everyone knows who has ever looked out of a window. Women who wear
glasses for minor defects of vision often observe that they are made
more or less color-blind by them, and in a shop one may note that
they remove them when they want to match samples. If the sight is
seriously defective, the color may be seen better with glasses than
without them.
That
glasses must injure the eye is evident from the facts given in the
preceding chapter. One cannot see through them unless one produces
the degree of refractive error which they are designed to
correct. But refractive errors, in the eye which is left to itself,
are never constant. If one secures good vision by the aid of concave,
or convex, or astigmatic lenses, therefore, it means that one is
maintaining constantly a degree of refractive error which otherwise
would not be maintained constantly. It is only to be expected that
this should make the condition worse, and it is a matter of common
experience that it does. After people once begin to wear glasses
their strength, in most cases, has to be steadily increased in
order to maintain the degree of visual acuity secured by the aid of
the first pair.
Persons
with presbyopia who put on glasses because they cannot read fine
print too often find that after they have worn them for a time they
cannot, without their aid, read the larger print that was perfectly
plain to them before. A person with myopia of 20/ 70 who puts on
glasses giving him a vision of 20/20 may find that in a week's time
his unaided vision has declined to 20/200, and we have the testimony
of Dr. Sidler-Huguenin, of Zurich,(1) that of the thousands of myopes
treated by him the majority grew steadily worse, in spite of all the
skill he could apply to the fitting of glasses for them.
When
people break their glasses and go without them for a week or two,
they frequently observe that their sight has improved. As a matter of
fact the sight always improves, to a greater or less degree, when
glasses are discarded, although the fact may not always be noted.
That
the human eye resents glasses is a fact which no one would attempt to
deny. Every oculist knows that patients have to "get used"
to them, and that sometimes they never succeed in doing so. Patients
with high degrees of myopia and hypermetropia have great difficulty
in accustoming themselves to the full correction, and often are
never able to do so. The strong concave glasses required by myopes of
high degree make all objects seem much smaller than they really are,
while convex glasses enlarge them. - These are unpleasantnesses that
cannot be overcome.
Patients
with high degrees of astigmatism suffer some very disagreeable
sensations when they first put on glasses, for which reason they are
warned by one of the "Conservation of Vision" leaflets
published by the Council on Health and Public Instruction of the
American Medical Association to "get used to them at home before
venturing where a misstep might cause a serious accident."(2)
Usually these difficulties are overcome, but often they are not,
and it sometimes happens that those who get on fairly well with their
glasses in the daytime never succeeded in getting used to them at
night.
All
glasses contract the field of vision to a greater or less
degree. Even with very weak glasses patients are unable to see
distinctly unless they look through the center of the lenses, with
the frames at right angles to the line of vision; and not only is
their vision lowered if they fail to do this, but annoying nervous
symptoms, such as dizziness and headache, are sometimes produced.
Therefore they are unable to turn their eyes freely in different
directions. It is true that glasses are now ground in such a way that
it is theoretically possible to look through them at any angle, but
practically they seldom accomplish the desired result.
The
difficulty of keeping the glass clear is one of the minor discomforts
of glasses, but nevertheless a most annoying one. On damp and
rainy days the atmosphere clouds them. On hot days the perspiration
from the body may have a similar effect. On cold days they are often
clouded by the moisture of the breath. Every day they are so subject
to contamination by dust and moisture and the touch of the fingers
incident to unavoidable handling that it is seldom they afford
an absolutely unobstructed view of the objects regarded.
Reflections
of-strong light from eyeglasses are often very annoying, and in the
street may be very dangerous.
Soldiers,
sailors, athletes, workmen and children have great difficulty with
glasses because of the activity of their lives, which not only leads
to the breaking of the lenses, but often throws them out of focus,
particularly in the case of eyeglasses worn for astigmatism.
The
fact that glasses are very disfiguring may seem a matter unworthy of
consideration in a medical publication; but mental discomfort does
not improve either the general health or the vision, and while we
have gone so far toward making a virtue of what we conceive to be
necessity that some of us have actually come to consider glasses
becoming, huge round lenses in ugly tortoiseshell frames being
positively fashionable at the present time, there are still
some unperverted minds to which the wearing of glasses is mental
torture and the sight of them upon others far from agreeable. Most
human beings are, unfortunately, ugly enough without- putting glasses
upon them, and to disfigure any of the really beautiful faces that we
have with such contrivances is surely as bad as putting an import tax
upon art. As for putting glasses upon a child it is enough to make
the angels weep.
Up
to a generation ago glasses were used only as an aid to defective
sight, but they are now prescribed for large numbers of persons
who can see as well or better without them. As explained in Chapter
I, the hypermetropic eye is believed to be capable of correcting its
own difficulties to some extent by altering the curvature of the
lens, through the activity of the ciliary muscle. The eye with simple
myopia is not credited with this capacity, because an increase in the
convexity of the lens, which is supposed to be all that is
accomplished by accommodative effort, would only increase the
difficulty; but myopia is usually accompanied by astigmatism,
and this, it is believed, can be overcome, in part, by
alterations in the curvature of the lens. Thus we are led by the
theory to the conclusion that an eye in which any error of refraction
exists is practically never free, while open, from abnormal
accommodative efforts. In other words, it is assumed that the
supposed muscle of accommodation has to bear, not only the normal
burden of changing the focus of the eye for vision at different
distances, but the additional burden of compensating for refractive
errors. Such adjustments, if they actually took place, would
naturally impose a severe strain upon the nervous system, and it is
to relieve this strain - which is believed to be the cause of a host
of functional nervous troubles - quite as much as to improve the
sight, that glasses are prescribed.
It
has been demonstrated, however, that the lens is not a factor, either
in the production of accommodation, or in the correction of
errors of refraction. Therefore under no circumstances can
there be a strain of the ciliary muscle to be relieved. It has also
been demonstrated that when the vision is normal no error of
refraction is present, and the extrinsic muscles of the eyeball are
at rest. Therefore, there can be no strain of the extrinsic
muscles to be relieved in these cases. When a strain of these muscles
does exist, glasses may correct its effects upon the refraction,
but the strain itself they cannot relieve. On the contrary, as has
been shown, they must make it worse. Nevertheless persons with
normal vision who wear glasses for the relief of a supposed muscular
strain are often benefited by them. This is a striking illustration
of the effect of mental suggestion, and plane glass, if it could
inspire the same faith, would produce the same result. In fact, many
patients have told me that they had been relieved of various
discomforts by glasses which I found to be simply plane glass. One of
these patients was an optician who had fitted the glasses himself and
was under no illusions whatever about them; yet he assured me
that when he didn't wear them he got headaches.
Some
patients are so responsive to mental suggestion that you can
relieve their discomfort, or improve their sight, with almost any
glasses you like to put on them. I have seen people with
hypermetropia wearing myopic glasses with a great deal of comfort,
and people with no astigmatism getting much satisfaction from
glasses designed for the correction of this defect.
Landolt
mentions the case of a patient who had for years worn prisms for
insufficiency of the internal recti, and who found them absolutely
indispensable for work, although the apices were toward the nose. The
prescription, which the patient was able to produce, called for
prisms adjusted in the usual manner, with the apices toward the
temples; but the optician had made a mistake which, owing to the
patient's satisfaction with the result, had never been discovered.
Landolt
explained the case by "the slight effect of weak prisms and the
great power of imagination";(3) and doubtless the benefit
derived from the glasses was real, resulting from the patient's great
faith in the specialist - described as "one of the most
competent of ophthalmologists" - who prescribed them.
Some
patients will even imagine that they see better with glasses that
markedly lower the vision. A number of years ago a patient for whom I
had prescribed glasses consulted an ophthalmologist whose
reputation was much greater than my own, and who gave him another
pair of glasses and spoke slightingly of the ones that I had
prescribed. The patient returned to me and told me how much
better he could see with the second pair of glasses than he did with
the first. I tested his vision with the new glasses, and found
that while mine had given him a vision of 20/20 those of my colleague
enabled him to see only 20/40. The simple fact was that he had been
hypnotized by a great reputation into thinking he could see better
when he actually saw worse; and it was hard to convince him that he
was wrong, although he had to admit that when he looked at the test
card he could see only half as much with the new glasses as with the
old ones.
When
glasses do not relieve headaches and other nervous symptoms it is
assumed to be because they were not properly fitted, and some
practitioners and their patients exhibit an astounding
degree of patience and perseverance in their joint attempts to arrive
at the proper prescription. A patient who suffered from severe
pains at the base of his brain was fitted sixty times by one
specialist alone, and had besides visited many other eye and nerve
specialists in this country and in Europe. He was relieved of the
pain in five minutes by the methods presented in this book, while his
vision, at the same time, became temporarily normal.
It
is fortunate that many people for whom glasses have been
prescribed refuse to wear them, thus escaping not only much
discomfort but much injury to their eyes. Others, having less
independence of mind, or a larger share of the martyr's spirit,
or having been more badly frightened by the oculists, submit to an
amount of unnecessary torture which is scarcely conceivable. One such
patient wore glasses for twenty-five years, although they did
not prevent her from suffering continual misery and lowered her
vision to such an extent that she had to look over the tops when she
wanted to see anything at a distance. Her oculist assured her that
she might expect the most serious consequences if she did not wear
the glasses, and was very severe about her practice of looking
over instead of through them.
As
refractive abnormalities are continually changing, not only from day
to day and from hour to hour, but from minute to minute, even under
the influence of atropine, the accurate fitting of glasses is, of
course; impossible. In some cases these fluctuations are so extreme,
or the patient so unresponsive to mental suggestion, that no relief
whatever is obtained from correcting lenses, which necessarily become
under such circumstances an added discomfort. At their best it
cannot be maintained that glasses are anything more than a very
unsatisfactory substitute for normal vision.
CITATIONS
1.
Archiv. f. Augenh., vol. lxxix, 1915, translated in Arch. Ophth.,
vol. xlv, No. 6, 1916.
2.
Lancaster: Wearing Glasses, p. 15.
3.Anomalies
of the Motor Apparatus of the Eye, System of Diseases of the Eye,
vol. iv, pp. 154-155.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
IX
THE CAUSE AND CURE OF ERRORS OF REFRACTION
It
has been demonstrated in thousands of cases that all abnormal action
of the external muscles of the eyeball is accompanied by a strain or
effort to see, and that with the relief of this strain the action of
the muscles becomes normal and all errors of refraction disappear.
The eye may be blind, it may be suffering from atrophy of the optic
nerve, from cataract, or disease of the retina; but so long as it
does not try to see, the external muscles act normally and there is
no error of refraction. This fact furnishes us with the means by
which all these conditions, so long held to be incurable, may be
cured.

Fig.
34. Straining to See at the Near-Point
Produces Hypermetropia -- Patient reading fine print in a good
light at thirteen inches, the object of vision being placed above the
eye so as to be out of the line of the camera. Simultaneous
retinoscopy indicated that the eye was focused
at
thirteen inches. The glass was used with the retinoscope to determine
the amount of the refraction. When the room was darkened the patient
failed to read the fine print at thirteen inches and the retinoscope
indicated that the eye was focused at a greater distance. When a
conscious strain of considerable degree was made to see, the eye
became hypermetropic.

Fig.
35. Myopia Produced by Unconscious Strain to See at the Distance
is Increased by Conscious Strain.
No.
1. - Normal vision.
No.
2. - Same subject four years later with myopia. Note the strained
expression.
No.
3. - Myopia increased by conscious effort to see a distant object.
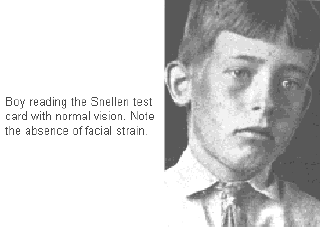
Fig.
36. Immediate Production of Myopia and Myopic Astigmatism in Eyes
Previously Normal by Strain to See at the Distance --
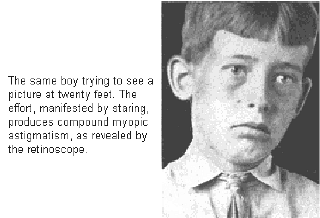
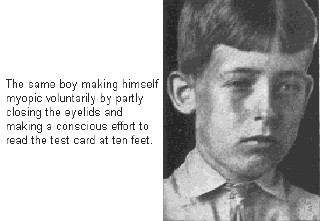
It
has also been demonstrated that for every error of refraction there
is a different kind of strain. The study of images reflected from
various parts of the eyeball confirmed what had previously been
observed, namely, that myopia (or a lessening of hypermetropia) is
always associated with a strain to see at the distance, while
hypermetropia (or/ a lessening of myopia) is always associated with a
strain to see at the nearpoint; and the fact can be verified in a:
few minutes by anyone who knows how to- use a retinoscope, provided
only that the instrument is not brought nearer to the subject than
six feet.
In
an eye with previously normal vision a strain to see near objects
always results in the temporary production of hypermetropia in one or
all meridians. That is, the eye either becomes entirely
hypermetropic, or some form of astigmatism is produced of which
hypermetropia forms a part. In the hypermetropic eye the
hypermetropia is increased in one or all meridians. When the myopic
eye strains to see a near object the myopia is lessened and
emmetropia(1) may be produced, the eye being focussed for
parallel rays while still trying to see at the near-point. In some
cases the emmetropia may even pass over into hypermetropia in one or
all meridians.
All
these changes are accompanied by evidences of increasing strain, in
the form of eccentric fixation (see Chapter XI) and lowered vision;
but, strange to say, pain and fatigue are usually relieved to a
marked degree. If, on the contrary, the eye with previously normal
vision strains to see at the distance, temporary myopia is
always produced in one or all meridians, and if the eye - is already
myopic, the myopia is increased.
If
the hypermetropic eye strains to see a distant object, pain and
fatigue may be produced or increased; but the hypermetropia and the
eccentric fixation are lessened-and the vision improves. This
interesting result, it will be noted, is the exact contrary of what
we get when the myope strains to see at the near-point. In some cases
the hypermetropia is completely relieved, and emmetropia is
produced, with a complete disappearance of all evidences of
strain. This condition may then pass over into myopia, with an
increase of strain as the myopia increases.
In
other words the eye which strains to see at the nearpoint becomes
flatter than it was before, in one or all meridians. If it was
elongated to start with, it may pass from this condition through
emmetropia, in which it is spherical, to hypermetropia, in which it
is flattened; and if these changes take place unsymmetrically,
astigmatism will be produced in connection with the other
conditions.
The
eye which strains to see at the distance, on the contrary, becomes
longer than it was before in one or all meridians, and may pass from
the flattened condition of hypermetropia, through emmetropia, to
the elongated condition of myopia. If these changes take place
unsymmetrically, astigmatism will again be produced in
connection with the other conditions.
What
has been said of the normal eye applies equally to eyes from which
the lens has been removed. This operation produces usually a
condition of hypermetropia; but when there has previously been a
condition of high myopia the removal of the lens may not be
sufficient to correct it, and the eye may still remain myopic. In the
first case a strain to see at the distance lessens the hypermetropia,
and a strain to see at the near-point increases it; in the second a
strain to see at the distance increases the myopia, and a strain to
see at the nearpoint lessens it. For a longer or shorter period after
the removal of the lens many aphakic eyes strain to see at the
near-point, producing so much hypermetropia that the patient cannot
read ordinary print, and the power of accommodation appears to have
been completely lost. Later, when the patient becomes accustomed
to the situation, this strain is often relieved, and the eye becomes
able to focus accurately upon near objects. Some rare cases have also
been observed in which a measure of good vision both for distance and
the nearpoint was obtained without glasses, the eyeball elongating
sufficiently to compensate, to some degree, for the loss of the lens.
The
phenomena associated with strain in the human eye have also been
observed in the eyes of the lower animals. I have made many dogs
myopic by inducing them to strain to see a distant object. One very
nervous dog, with normal refraction, as demonstrated by the
retinoscope, was allowed to smell a piece of meat. He became very
much excited, pricked up his ears, arched his eyebrows and wagged his
tail. The meat was then removed to a distance of twenty feet. The dog
looked disappointed, but didn't lose interest. While he was watching
the meat it was dropped into a box. A worried look came into his
eyes. He strained to see what had become of it, and the retinoscope
showed that he had become myopic. This experiment, it should be
added, would succeed only with an animal possessing two active
oblique muscles. Animals in which one of these muscles is absent or
rudimentary are unable to elongate the eyeball under any
circumstances.
Primarily
the strain to see is a strain of the mind, and, as in all cases in
which there is a strain of the mind, there is a loss of mental
control. Anatomically the results of straining to see at a distance
may be the same as those of regarding an object at the near point
without strain; but in one case the eye does what the mind desires,
and in the other it does not.
These
facts appear sufficiently to explain why visual acuity declines as
civilization advances. Under the conditions of civilized life men's
minds are under a continual strain. They have more things to worry
them than uncivilized man had, and they are not obliged to keep cool
and collected in order that they may see and do other things upon
which existence depends. If he allowed himself to get nervous,
primitive man was promptly eliminated; but civilized man survives and
transmits his mental characteristics to posterity. The lower
animals when subjected to civilized conditions respond to them
in precisely the same way as do human creatures. I have examined
many domestic and menagerie animals, and have found them, in many
cases, myopic, although they neither read, nor write, nor sew, nor
set type.
Fig.
37. Myopic Astigmatism Comes and Goes According as
the
Subject Looks at Distant Objects With or Without Strain --
No.
1. - Patient regarding the Snellen test card at ten feet without
effort and reading the bottom line with normal vision.
No.
2. - The same patient making an effort to see a picture at twenty
feet. The retinoscope indicated compound myopic astigmatism.
Fig.
38. This Patient Had Had the Lens of the Right Eye Removed for
Cataract and Was Wearing an Artificial Eye in the Left Socket.
The
Removal of the Lens Created a Condition of Hypermetropia Which
Was Corrected by a Convex Glass of Ten Diopters.
No.
1. - The patient is reading the Snellen test card at twenty feet
with normal vision.
No.
2. - She is straining to see the test card at the same distance, and
her hypermetropia is lessened by two diopters so that her glass
now overcorrects it and she cannot see the card perfectly.
No.
3. - With a convex reading glass of thirteen diopters the right eye
is focussed accurately at thirteen inches.
No.
4. - The patient is straining to see at the same distance and her
hypermetropia is so increased that in order to read she would require
a glass of fifteen diopters. On the basis of the accepted theory
that the power of accommodation is wholly destroyed by the removal of
the lens these changes in the refraction would have been impossible.
The experiment was repeated several times and it was found that the
error of refraction produced by straining to see varied, being
sometimes more and sometimes less than two diopters.
Fig.
39. A Family Group Strikingly Illustrating the Effect of the Mind
Upon the Vision --
No.
1. - Girl of four with normal eyes.
No.
2. - The child's mother with myopia.
No.
3. - The same girl at nine with myopia. Note that her expression has
completely changed, and is now exactly like her mother's.
Nos.
4, 5 and 6. - The girl's brother at two, six and eight. His eyes are
normal in all three pictures. The girl has either inherited her
mother's disposition to take things hard, or has been injuriously
effected by her personality of strain. The boy has escaped both
influences. In view of the prevailing theories about the relation of
heredity to myopia, this picture is particularly interesting.

Fig.
40. Myopes Who Never Went to School, or Read in the Subway
No.
1. - Myopic elephant in the Central Park Zoo, New York thirtynine
years old. Young elephants and other young animals were found to have
normal vision. (not shown)
No.
2. - Cape buffalo with myopia, Central Park Zoo.
No.
3. - Myopic monkey, also in the Central Park Zoo.
No.
4. - Pet dog with myopia which progressed from year to year.
A
decline in visual acuity at the distance, however, is no more a
peculiarity of civilization than is a similar decline at the
near-point. Myopes, although they see better at the near-point than
they do at the distance, never see as well as does the eye with
normal sight; and in hypermetropia, which is more common than myopia,
the sight is worse at the near-point than at the distance.
The
remedy is not to avoid either near work or distant vision, but to get
rid of the mental strain which underlies the imperfect functioning of
the eye at both points; and it has: been demonstrated in thousands of
cases that this can always be done.
Fortunately,
all persons are able to relax under certain conditions at will. In
all uncomplicated errors of refraction the strain to see can be
relieved, temporarily, by having the patient look at a blank wall
without trying to see. -To secure permanent relaxation sometimes
requires considerable time and much ingenuity. The same method cannot
be used with everyone. The ways in which people strain to see are
infinite, and the methods used to relieve the strain must be almost
equally varied. Whatever the method that brings most relief, however,
the end is always the same, namely relaxation. By constant repetition
and frequent demonstration and by all means possible, the fact must
be impressed upon the patient that perfect sight can be obtained only
by relaxation. Nothing else matters.
Most
people, when told that rest, or relaxation, will cure their eye
troubles, ask why sleep does not do so. The answer to this question
was given in Chapter VII. The eyes are rarely, if ever, completely
relaxed in sleep, and if they are under a strain when the subject is
awake, that strain will certainly be continued during sleep, to a
greater or less degree, just as a strain of other parts of the body
is continued.
The
idea that it rests the eyes not to use them is also erroneous. The
eyes were made to see with, and if when they are open they do not
see, it is because they are under such a strain and have such a great
error of refraction that they cannot see. Near vision, although
accomplished by a muscular act, is no more a strain on them than is
distant vision, although accomplished without the intervention of the
muscles. The use of the muscles does not necessarily produce
fatigue. Some men can run for hours without becoming tired. Many
birds support themselves upon one foot during sleep, the toes tightly
clasping the swaying bough and the muscles remaining unfatigued by
the apparent strain. Fabre tells of an insect which hung back
downward for ten months from the roof of its wire cage, and in that
position performed all the functions of life, even to mating and
laying its eggs. Those who fear the effect of civilization, with its
numerous demands for near vision, upon the eye may take courage from
the example of this marvelous little animal which, in a state of
nature, hangs by its feet only at intervals, but in captivity can do
it for ten months on end, the whole of its life's span, apparently
without inconvenience or fatigue.(2)
The
fact is that when the mind is at rest nothing can tire the eyes, and
when the mind is under a strain nothing can rest them. Anything that
rests the mind will benefit the eyes. Almost everyone has observed
that the eyes tire less quickly when reading an interesting book than
when perusing something tiresome or difficult to comprehend. A
schoolboy can sit up all night reading a novel without even thinking
of his eyes, but if he tried to sit up all night studying his lessons
he would soon find them getting very tired. A child whose vision was
ordinarily so acute that she could see the moons of Jupiter with the
naked eye became myopic when asked to do a sum in mental arithmetic,
mathematics being a subject which was extremely distasteful to her.
Sometimes the conditions which produce mental relaxation are very
curious. One patient, for instance, was able to correct her error of
refraction when she looked at the test card with her body bent over
at an angle of about forty-five degrees, and the relaxation continued
after she had assumed the upright position. Although the position was
an unfavorable one, she had somehow got the idea that it improved her
sight, and therefore it did so.

Fig.
41. - One of Many Thousands of Patients Cured of Errors of Refraction
by the Methods Presented in This Book
No.
1. - Man of thirty-six, 1902, wearing glasses for myopia. Note the
appearance of effort in his eyes. He was relieved in 1904 by means of
exercises in distant vision and obtained normal sight without
glasses.
No.
2. - The same man five years later. No relapse.
The
time required to effect a permanent cure varies greatly with
different individuals. In some cases five, ten, or fifteen minutes is
sufficient, and I believe the time is coming when it will be possible
to cure everyone quickly. It is only a question of accumulating more
facts, and presenting these facts in such a way that the patient can
grasp them quickly. At present, however, it is often necessary to
continue the treatment for weeks and months, although the error of
refraction may be no greater nor of longer duration than in those
cases that are cured quickly. In most cases, too, the treatment must
be continued for a few minutes every day to prevent relapse. Because
a familiar object tends to relax the strain to see, the daily reading
of the Snellen test card is usually sufficient for this purpose. It
is also useful, particularly when the vision at the near-point is
imperfect, to read fine print every day as close to the eyes as it
can be done. When a cure is complete it is always permanent; but
complete cures, which mean the attainment, not of what is ordinarily
called normal sight, but of a measure of telescopic and microscopic
vision, are very rare. Even in these cases, too, the treatment can be
continued with benefit; for it is impossible to place limits to the
visual powers of man, and no matter how good the sight, it is always
possible to improve it.
Daily
practice of the art of vision is also necessary to prevent those
visual lapses to which every eye is liable, no matter how good its
sight may ordinarily be. It is true that no system of training will
provide an absolute safeguard against such lapses in all
circumstances; but the daily reading of small distant, familiar
letters will do much to lessen the tendency to strain when disturbing
circumstances arise, and all persons upon whose eyesight the safety
of others depends should be required to do this.
Generally
persons who have never worn glasses are more easily cured than those
who have, and glasses should be discarded at the beginning of the
treatment. When this cannot be done without too great discomfort, or
when the patient has to continue his work during the treatment and
cannot do so without glasses, their use must be permitted for a time;
but this always delays the cure. Persons of all ages have been
benefited by this treatment of errors of refraction by relaxation;
but children usually, though not invariably, respond much more
quickly than adults. If they are under twelve years of age, or even
under sixteen, and have never worn glasses, they are usually cured in
a few days, weeks, or months, and always within a year, simply by
reading the Snellen test card every day.
CITATIONS
1.
Emmetropia (from the Greek emmetros, in measure, and ops,
the eye) is that condition of the eye in which it is focussed for
parallel rays. This constitutes normal vision at the distance but is
an error of refraction when it occurs at the near-point.
2.
The Wonders of Instinct, English translation by de Mattos and Miall,
1918, pp. 36-38.
THE CURE OF
IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
X
STRAIN
Temporary
conditions may contribute to the strain to see which results in the
production of errors of refraction; but its foundation lies in wrong
habits of thought. In attempting to relieve it the physician has
continually to struggle against the idea that to do anything well
requires effort. This idea is drilled into us from our cradles. The
whole educational system is based upon it; and in spite of the
wonderful results attained by Montessori through the total
elimination of every species of compulsion in the educational
process, educators who call themselves modern still cling to the
club, under various disguises, as a necessary auxiliary to the
process of imparting knowledge.
It
is as natural for the eye to see as it is for the mind to acquire
knowledge, and any effort in either case is not only useless, but
defeats the end in view. You may force a few facts into a child's
mind by various kinds of compulsion, but you cannot make it learn
anything. The facts remain, if they remain at all, as dead lumber in
the brain. They contribute nothing to the vital processes of thought;
and because they were not acquired naturally and not assimilated,
they destroy the natural impulse of the mind toward the acquisition
of knowledge, and by the time the child leaves school or college, as
the case may be, it not only knows nothing but is, in the majority of
cases, no longer capable of learning.
In
the same way you may temporarily improve the sight by effort, but you
cannot improve it to normal, and if the effort is allowed to become
continuous, the sight will steadily deteriorate and may eventually
be destroyed. Very seldom is the impairment or destruction of vision
due to any fault in the construction of the eye. Of two
equally good pairs of eyes one will retain perfect sight to the end
of life, and the other will lose it in the kindergarten, simply
because one looks at things without effort and the other does not.
The
eye with normal sight never tries to see. If for any reason, such as
the dimness of the light, or the distance of the object, it cannot
see a particular point, it shifts to another. It never tries to bring
out the point by staring at it, as the eye with imperfect sight is
constantly doing.
Whenever
the eye tries to see, it at once ceases to have normal vision. A
person may look at the stars with normal vision; but if he tries to
count the stars in any particular constellation, he will probably
become myopic, because the attempt to do these things usually results
in an effort to see. A patient was able to look at the letter K on
the Snellen test card with normal vision, but when asked to count its
twentyseven corners he lost it completely.
It
obviously requires a strain to fail to see at the distance, because
the eye at rest is adjusted for distant vision. If one does anything
when one wants to see at the distance, one must do the wrong thing.
The shape of the eyeball cannot be altered during distant vision
without strain. It is equally a strain to fail to see at the
near-point, because when the muscles respond to the mind's desire
they do it without strain. Only by an effort can one prevent the eye
from elongating at the near-point.
The
eye possesses perfect vision only when it is absolutely at rest. Any
movement, either in the organ or the object of vision, produces an
error of refraction. With the retinoscope it can be demonstrated
that even the necessary movements of the eyeball produce a slight
error of refraction, and the moving pictures have given us a
practical demonstration of the fact that it is impossible to see
a moving object perfectly. When the movement of the object of vision
is sufficiently slow, the resulting impairment of vision is so
slight as to be inappreciable, just as the errors of refraction
produced by slight movements of the eyeball are inappreciable; but
when objects move very rapidly they can be seen only as a blur. For
this reason it has been found necessary to arrange the machinery for
exhibiting moving pictures in such a way that each picture is halted
for a twenty-fourth of a second, and screened while it is moving into
place. Moving pictures, accordingly, are never seen in motion.
The
act of seeing is passive. Things are seen, just as they are felt, or
heard, or tasted, without effort or volition on the part of the
subject. When sight is perfect the letters on the test card are
waiting, perfectly black and perfectly distinct, to be recognized.
They do not have to be sought; they are there. In imperfect sight
they are sought and chased. The eye goes after them. An effort is
made to see them.
The
muscles of the body are supposed never to be at rest. The
blood-vessels, with their muscular coats, are never at rest. Even in
sleep thought does not cease. But the normal condition of the nerves
of sense - of hearing, sight, taste, smell and touch - is one of
rest. They can be acted upon; they cannot act. The optic nerve, the
retina and the visual centers of the brain are as passive as the
finger-nail. They have nothing whatever in their structure that makes
it possible for them to do anything, and when they are the subject of
effort from outside sources their efficiency is always impaired.
The
mind is the source of all such efforts from outside sources brought
to bear upon the eye. Every thought of effort in the mind, of
whatever sort, transmits a motor impulse to the eye; and every such
impulse causes a deviation from the normal in the shape of the
eyeball and lessens the sensitiveness of the center of sight. If
one wants to have perfect sight, therefore, one must have no thought
of effort in the mind. Mental strain of any kind always produces a
conscious or unconscious eyestrain and if the strain takes the form
of an effort to see, an error of refraction is always produced. A
schoolboy was able to read the bottom line of the Snellen test
card at ten feet, but when the teacher told him to mind what he was
about he could not see the big C.(1) Many children can see perfectly
so long as their mothers are around; but if the mother goes out of
the room, they may at once become myopic, because of the strain
produced by fear. Unfamiliar objects produce eyestrain and a
consequent error of refraction, because they first produce mental
strain. A person may have good vision when he is telling the truth;
but if he states what is not true, even with no intent to deceive, or
if he imagines what is not true, an error of refraction will be
produced, because it is impossible to state or imagine what is
not true without an effort.
I
may claim to have discovered that telling lies is bad for the eyes,
and whatever bearing this circumstance may have upon the
universality of defects of vision, the fact can easily be
demonstrated. If a patient can read all the small letters on the
bottom line of the test card, and either deliberately or carelessly
miscalls any of them, the retinoscope will indicate an error of
refraction. In numerous cases patients have been asked to state their
ages incorrectly, or to try to imagine that they were a year older or
a year younger than they actually were, and in every case when they
did this the retinoscope indicated an error of refraction. A patient
twenty-five years old had no error of refraction when he looked at a
blank wall without trying to see; but if he said he was twenty-six,
or if someone else said he was twenty-six, or if he tried to imagine
that he was twenty-six, he became myopic. The same thing happened
when he stated or tried to imagine that he was twenty-four. When he
stated or remembered the truth his vision was normal, but when he
stated or imagined an error he had an error of refraction.
Two
little girl patients arrived one after the other one day, and the
first accused the second of having stopped at Huyler's for an
ice-cream soda, which she had been instructed not to do, being
somewhat too much addicted to sweets. The second denied the charge,
and the first, who had used the retinoscope and knew what it did to
people who told lies, said:
"Do
take the retinoscope and find out."
I
followed the suggestion, and having thrown the light into the second
child's eyes, I asked:
"Did
you go to Huyler's?"
"Yes,"
was the response, and the retinoscope indicated no error of
refraction.
"Did
you have an ice-cream soda?"
"No,"
said the child; but the telltale shadow moved in a direction opposite
to that of the mirror, showing that she had become myopic and
was not telling the truth.
The
child blushed when I told her this and acknowledged that the
retinoscope was right; for she had heard of the ways of the uncanny
instrument before and did not know what else it might do to her if
she said any thing more that was not true.
So
sensitive is this test that if the subject, whether his vision
is ordinarily normal or not, pronounces the initials of his name
correctly while looking at a blank surface without trying to see,
there will be no error of refraction; but if he miscalls one initial,
even without any consciousness of effort, and with full knowledge
that he is deceiving no one, myopia will be produced.
Mental
strain may produce many different kinds of eyestrain. According to
the statement of most authorities there is only one kind of
eyestrain, an indefinite thing resulting from so-called overuse
of the eyes, or an effort to overcome a wrong shape of the eyeball.
It can be demonstrated, however, that there is not only a different
strain for each different error of refraction, but a different
strain for most abnormal conditions of the eye. The strain that
produces an error of refraction is not the same as the strain that
produces a squint, or a cataract,(1) or glaucoma,(3) or amblyopia,(4)
or inflammation of the conjunctiva(5) or of the margin of the lids,
or disease of the optic nerve or retina. All these conditions
may exist with only a slight error of refraction, and while the
relief of one strain usually means the relief of any others that may
coexist with it, it sometimes happens that the strain associated with
such conditions as cataract and glaucoma is relieved without the
complete relief of the strain that causes the error of refraction.
Even the pain that so often accompanies errors of refraction is never
caused by the same strain that causes these errors. Some myopes
cannot read without pain or discomfort, but most of them suffer
no inconvenience. When the hypermetrope regards an object at the
distance the hypermetropia is lessened, but pain and discomfort may
be increased. While there are many strains, however, there is only
one cure for all of them. namely, relaxation.
The
health of the eye depends upon the blood, and, circulation is very
largely influenced by thought. When thought is normal - that is, not
attended by any excitement or strain - the circulation in the brain
is normal, the supply of blood to the optic nerve and the visual
centers is normal, and the vision is perfect. When thought is
abnormal the circulation is disturbed, the supply of blood to the
optic nerve and visual centers is altered, and the vision lowered. We
can consciously think thoughts which disturb the circulation and
lower the visual power; we can also consciously think thoughts that
will restore normal circulation, and thereby cure, not only all
errors of refraction, but many other abnormal conditions of the eyes.
We cannot by any amount of effort make ourselves see, but by learning
to control our thoughts we can accomplish that end indirectly.
You
can teach people how to produce any error of refraction, how to
produce a squint, how to see two images of an object, one above
another, or side by side, or at any desired angle from one another,
simply by teaching them how to think in a particular way. When the
disturbing thought is replaced by one that relaxes, the squint
disappears, the double vision and the errors of refraction are
corrected; and this is as true of abnormalities of long standing as
of those produced voluntarily. No matter what their degree or their
duration their cure is accomplished just as soon as the patient
| is able to secure mental control. The cause of any error I of
refraction, of a squint, or of any other functional disturbance
of the eye, is simply a thought - a wrong thought - and the cure is
as quick as the thought that relaxes. In a fraction of a second the
highest degrees of refractive error may be corrected, a squint may
disappear, or the blindness of amblyopia may be relieved. If the
relaxation is only momentary, the correction is momentary. When
it becomes permanent, the correction is permanent.
This
relaxation cannot, however, be obtained by any sort of effort. It is
fundamental that patients should understand this; for so long as they
think, consciously or unconsciously, that relief from strain may be
obtained by another strain their cure will be delayed.
CITATIONS
1
In this case and others to be mentioned later, the large letter at
the top of the card read by the eye with normal vision at two hundred
feet, was a "C."
2.
An opacity of the lens.
3.
A condition in which the eyeball becomes abnormally hard.
4.
A condition in which there is a decline of vision without apparent
cause.
5.
A membrane covering the inner surface of the eyelid and the visible
part of the white of the eye.
THE CURE OF
IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XI
CENTRAL FIXATION
The
eye is a miniature camera, corresponding in many ways very exactly to
the inanimate machine used in photography. In one respect, however,
there is a great difference between the two instruments. The
sensitive plate of the camera is equally sensitive in every part; but
the retina has a point of maximum sensitiveness, and every other part
is less sensitive in proportion as it is removed from that point.
This point of maximum sensitiveness is called the "fovea
centralis," literally the "central pit."
The
retina, although it is an extremely delicate membrane, varying in
thickness from one-eightieth of an inch to less than half that
amount, is highly complex. It is composed of nine layers, only one of
which is supposed to be capable of receiving visual impressions. This
layer is composed of minute rodlike and conical bodies which
vary in form and are distributed very differently in its different
parts. In the center of the retina is a small circular elevation
known, from the yellow color which it assumes in death and sometimes
also in life, as the "macula lutea," literally the "yellow
spot." In the center of this spot is the fovea, a deep
depression of darker color. In the center of this depression there
are no rods, and the cones are elongated and pressed very closely
together. The other layers, on the contrary, become here extremely
thin, or disappear altogether, so that the cones are covered
with barely perceptible traces of them. Beyond the center of the
fovea the cones become thicker and fewer and are interspersed with
rods, the number of which increases toward the margin of the retina.
The precise function of these rods and cones is not clear; but it is
a fact that the center of the fovea, where all elements except the
cones and their associated cells practically disappear, is the seat
of the most acute vision. As we withdraw from this spot, the
acuteness of the visual perceptions rapidly decreases. The eye with
normal vision, therefore, sees one part of everything it looks at
best, and everything else worse, in proportion as it is removed from
the point of maximum vision; and it is an invariable symptom of
all abnormal conditions of the eyes, both functional and organic,
that this central fixation is lost.
These
conditions are due to the fact that when the sight is normal the
sensitiveness of the fovea is normal, but when the sight is
imperfect, from whatever cause, the sensitiveness of the fovea is
lowered, so that the eye sees equally well, or even better, with
other parts of the retina. Contrary to what is generally believed,
the part seen best when the sight is normal is extremely small. The
text-books say that at twenty feet an area having a diameter of half
an inch can be seen with maximum vision, but anyone who tries at this
distance to see every part of even the smallest letters of the
Snellen test card - the diameter of which may be less than a quarter
of an inch - equally well at one time will immediately become myopic.
The fact is that the nearer the point of maximum vision approaches
a mathematical point, which has no area, the better the sight.
The
cause of this loss of function in the center of sight is mental
strain; and as all abnormal conditions of the eyes, organic as well
as functional, are accompanied by mental strain, all such
conditions must necessarily be accompanied by loss of central
fixation. When the mind is under a strain the eye usually goes
more or less blind. The center of sight goes blind first, partially
or completely, according to the degree of the strain, and if the
strain is great enough the whole or the greater part of the retina
may be involved. When the vision of the center of sight has been
suppressed, partially or completely, the patient can no longer see
the point which he is looking at best, but sees objects not regarded
directly as well, or better, because the sensitiveness of the
retina has now become approximately equal in every part, or is even
better in the outer part than in the center. Therefore in all cases
of defective vision the patient is unable to see best where he is
looking.
This
condition is sometimes so extreme that the patient may look as far
away from an object as it is possible to see it, and yet see it just
as well as when looking directly at it. In one case it had gone so
far that the patient could see only with the edge of the retina on
the nasal side. In other words, she could not see her fingers in
front of her face, but could see them if held at the outer side of
her eye. She had only a slight error of refraction, showing that
while every error of refraction is accompanied by eccentric fixation,
the strain which causes the one condition is different from that
which produces the other. The patient had been examined by
specialists in this country and Europe, who attributed her blindness
to disease of the optic nerve or brain; but the fact that vision was
restored by relaxation demonstrated that the condition had been due
simply to mental strain.
Eccentric
fixation, even in its lesser degrees, is so unnatural that great
discomfort, or even pain, can be produced in a few seconds by trying
to see every part of an area three or four inches in extent at twenty
feet, or even less, or an area of an inch or less at the near-point,
equally well at one time, while at the same time the retinoscope will
demonstrate that an error of refraction has been produced. This
strain, when it is habitual, leads to all sorts of abnormal
conditions and is, in fact, at the bottom of most eye troubles, both
functional and organic. The discomfort and pain may be absent,
however, in the chronic condition, and it is an encouraging symptom
when the patient begins to experience them.
When
the eye possesses central fixation it not only possesses perfect
sight, but it is perfectly at rest and can be used indefinitely
without fatigue. It is open and quiet; no nervous movements are
observable; and when it regards a point at the distance the
visual axes are parallel. In other words, there are no muscular
insufficiencies. This fact is not generally known. The textbooks
state that muscular insufficiencies occur in eyes having normal
sight, but I have never seen such a case. The muscles of the face and
of the whole body are also at rest, and when the condition is
habitual there are no wrinkles or dark circles around the eyes.
In
most cases of eccentric fixation, on the contrary, the eye quickly
tires, and its appearance, with that of the face, is expressive of
effort or strain. The ophthalmoscope(1) reveals that the eyeball
moves at irregular intervals, from side to side, vertically or in
other directions. These movements are often so extensive as to
be manifest by ordinary inspection, and are sometimes sufficiently
marked to resemble nystagmus.(2) Nervous movements of the
eyelids may also be noted, either by ordinary inspection, or by
lightly touching the lid of one eye while the other regards an object
either at the near-point or the distance. The visual axes are never
parallel, and the deviation from the normal may become so marked as
to constitute the condition of squint. Redness of the conjunctiva and
of the margins of the lids, wrinkles around the eyes, dark circles
beneath them and tearing are other symptoms of eccentric fixation.
Eccentric
fixation is a symptom of strain, and is relieved by any method that
relieves strain; but in some cases the patient is cured just as soon
as he is able to demonstrate the facts of central fixation. When he
comes to realize, through actual demonstration of the fact,
that he does not see best where he is looking, and that when he looks
a sufficient distance away from a point he can see it worse than
when he looks directly at it, he becomes able, in some way, to reduce
the distance to which he has to look in order to see worse, until he
can look directly at the top of a small letter and see the
bottom worse, or look at the bottom and see the top worse. The
smaller the letter regarded in this way, or the shorter the distance
the patient has to look away from a letter in order to see the
opposite part indistinctly, the greater the relaxation and the
better the sight. When it becomes possible to look at the bottom
of a letter and see the top worse, or to look at the top and see the
bottom worse, it becomes possible to see the letter perfectly black
and distinct. At first such vision may come only in flashes. The
letter will come out distinctly for a moment and then disappear. But
gradually, if the practice is continued, central fixation will become
habitual.
Most
patients can readily look at the bottom of the big C and see the top
worse; but in some cases it is not only impossible for them to do
this, but impossible for them to let go of the large letters at
any distance at which they can be seen. In these extreme cases it
sometimes requires considerable ingenuity, first to demonstrate to
the patient that he does not see best where he is looking, and then
to help him to see an object worse when he looks away from it than
when he looks directly at it. The use of a strong light as one of the
points of fixation, or of two lights five or ten feet apart, has been
found helpful, the patient when he looks away from the light being
able to see it less bright more readily than he can see a black
letter worse when he looks away from it. It then becomes easier for
him to see the letter worse when he looks away from it. This method
was successful in the following case:
A
patient with vision of 3/200, when she looked at a point a few feet
away from the big C, said she saw the letter better than when she
looked directly at it. Her attention was called to the fact that her
eyes soon became tired and that her vision soon failed when she saw
things in this way. Then she was directed to look at a bright object
about three feet away from the card, and this attracted her
attention to such an extent that she became able to see the
large letter on the test card worse, after which she was able to look
back at it and see it better. It was demonstrated to her that she
could do one of two things: look away and see the letter better than
she did before, or look away and see it worse. She then became able
to see it worse all the time when she looked three feet away from it.
Next she became able to shorten the distance successively to two
feet, one foot, and six inches, with a constant improvement in
vision; and finally she became able to look at the bottom of the
letter and see the top worse, or look at the top and see the bottom
worse. With practice she became able to look at the smaller letters
in the same way, and finally she became able to read the ten line at
twenty feet. By the same method also she became able to read diamond
type, first at twelve inches and then at three inches. By these
simple measures alone she became able, in short, to see best where
she was looking, and her cure was complete.
The
highest degrees of eccentric fixation occur in the high degrees of
myopia, and in these cases, since the sight is best at the
near-point, the patient is benefited by practicing seeing worse at
this point. The distance can then be gradually extended until it
becomes possible to do the same thing at twenty feet. One patient
with a high degree of myopia said that the farther she looked away
from an electric light the better she saw it, but by alternately
looking at the light at the near-point and looking away from it
she became able, in a short time, to see it brighter when she looked
directly at it than when she looked away from it. Later she became
able to do the same thing at twenty feet, and then she experienced a
wonderful feeling of relief. No words, she said, could adequately
describe it. Every nerve seemed to be relaxed, and a feeling of
comfort and rest permeated her whole body. Afterward her progress was
rapid. She soon became able to look at one part of the smallest
letters on the card and see the rest worse, and then she became able
to read the letters at twenty feet.
On
the principle that a burnt child dreads the fire, some patients are
benefited by consciously making their sight worse. When they learn,
by actual demonstration of the facts, just how their visual defects
are produced, they unconsciously avoid the unconscious strain which
causes them. When the degree of eccentric fixation is not too extreme
to be increased;, therefore, it is a benefit to patients to teach
them how to increase it. When a patient has consciously lowered his
vision and produced discomfort and even pain by trying to see the big
C, or a whole line of letters, equally well at one time, he becomes
better able to correct the unconscious effort of the eye to see all
parts of a smaller area equally well at one time.
In
learning to see best where he is looking it is usually- l best for
the patient to think of the point not directly regarded as being seen
less distinctly than the point he is | looking at, instead of
thinking of the point fixed as being 1 seen best, as the latter
practice has a tendency, in most 11 cases, to intensify the
strain under which the eye is already laboring. One part of an object
is seen best only when the mind is content to see the greater part
of it indistinctly? and as the degree of relaxation increases, the
area of the part seen worse increases, until that seen best becomes
merely a point.
The
limits of vision depend upon the degree of central fixation. A
person may be able to read a sign half a mile away when he sees the
letters all alike, but when taught to see one letter best he will be
able to read smaller letters that he didn't know were there. The
remarkable vision of savages, who can see with the naked eye objects
for which most civilized persons require a telescope, is a matter of
central fixation. Some people can see the moons of Jupiter, with the
naked eye. It is not because of any superiority in the structure of
their eyes, but because they have attained a higher degree of central
fixation than most civilized persons do.
Not
only do all errors of refraction and all functional disturbances
of the eye disappear when it sees by central fixation, but many
organic conditions are relieved or cured. I am unable to set any
limits to its possibilities. I would not have ventured to predict
that glaucoma, incipient cataract and syphilitic iritis could be
cured by central fixation; but It is a fact that these conditions
have disappeared when central}fixation was attained. Relief was
often obtained in a few minutes, and, in rare cases, this relief was
permanent. Usually, however, a permanent cure required more prolonged
treatment. Inflammatory conditions of all kinds, including
inflammation of the cornea, iris, conjunctiva, the various coats of
the eyeball and even the optic nerve itself, have been benefited by
central fixation after other methods had failed. Infections, as well
as diseases caused by protein poisoning and the poisons of
typhoid fever, influenza, syphilis and gonorrhea, have also been
benefited by it. Even with a foreign body in the eye there is no
redness and no pain so long as central fixation is retained.
Since
central fixation is impossible without mental control, central
fixation of the eye means central fixation of the mind. It means,
therefore, health in all parts of the body, for all the operations of
the physical mechanism depend upon the mind. Not only the sight, but
all the other senses - touch, taste, hearing and smell - are
benefited by central fixation. All the vital processes -
digestion, assimilation, elimination, etc. - are improved by it. The
symptoms of functional and organic diseases arc relieved. The
efficiency of the mind is enormously increased. The benefits of
central fixation already observed are, in short, so great that the
subject merits further investigation.
CITATIONS
1.
A shorter movement can be noted when the observer watches the optic
nerve with the ophthalmoscope than when he views merely the
exterior of the eye.
2.
A condition in which there is a conspicuous and more or less rhythmic
movement of the eyeball from side to side.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XIII
MEMORY AS AN AID TO VISION
When
the mind is able to remember perfectly any phenomenon of the senses,
it is always perfectly relaxed. The sight is normal, if the eyes are
open; and when they are closed and covered so as to exclude all the
light, one sees a perfectly black field - that is nothing at all. If
you can remember the ticking of a watch, or an odor or a taste
perfectly, your mind is perfectly at rest, and you will see a perfect
black when your eyes are closed and covered. If your memory of a
sensation of touch could be equal to the reality, you would see
nothing but black when the light was excluded from your eyes. If you
were to remember a bar of music perfectly when your eyes were closed
and covered, you would see nothing but black. But in the case of any
of these phenomena it is not easy to test the correctness of the
memory, and the same is true of colors other than black. All other
colors, including white, are altered by the amount of light to which
they are exposed, and are seldom seen as perfectly as it is possible
for the normal eye to see them. But when the sight is normal, black
is just as black in a dim light as in a bright one. It is also just
as black at the distance as at the near-point, while a small area is
just as black as a large one, and, in fact, appears blacker. Black
is, moreover, more readily available than any other color. There is
nothing blacker than printer's ink, and that is practically
ubiquitous. By means of the memory of black, therefore, it is
possible to measure accurately one's own relaxation. If the color is
remembered perfectly, one is perfectly relaxed. If it is remembered
almost perfectly, one's relaxation is almost perfect. If it cannot be
remembered at all, one has very little or no relaxation.
By
means of simultaneous retinoscopy, these facts can be readily
demonstrated. An absolutely perfect memory is very rare, so much so
that it need hardly be taken into consideration; but a practically
perfect memory, or what might be called normal, is attainable by
every one under certain conditions. With such a memory of black, the
retinoscope shows that all errors of refraction are corrected. If the
memory is less than normal, the contrary will be the case. If it
fluctuates, the shadow of the retinoscope will fluctuate. The
testimony of the retinoscope is, in fact, more reliable than the
statements of the patient. Patients often believe and state that they
remember black perfectly, or normally, when the retinoscope indicates
an error of refraction; but in such cases it can usually be
demonstrated by bringing the test card to the point at which the
black letters can be seen best, that the memory is not equal to the
sight. That the color cannot be remembered perfectly when the
eyes and mind are under a strain, the reader can easily demonstrate
by trying to remember it when making a conscious effort to see - by
staring, partly closing the eyes, frowning, etc - or while trying to
see all the letters of a line equally well at one time. It will be
found that it either cannot be remembered at all under these
conditions, or that it is remembered very imperfectly.
When
the two eyes of a patient are different, it has been found that the
difference can be exactly measured by the length of time a black
period can be remembered, while looking at the Snellen test card,
with both eyes open, and with the better eye closed. A patient with
normal vision in the right eye and half-normal vision in the left
could, when looking at the test card with both eyes open, remember a
period for twenty seconds continuously; but with the better eye
closed, it could be remembered only ten seconds. A patient with
half-normal vision in the right eye and one-quarter normal in the
left could remember a period twelve seconds with both eyes open, and
only six seconds with the better eye closed. A third patient, with
normal sight in the right eye and vision of one-tenth in the left,
could remember a period twenty seconds with both eyes open, and only
two seconds when the better eye was closed. In other words, if the
right eye is better than the left, the memory is better when the
right eye is open than when only the left eye is open, the difference
being in exact proportion to the difference in the vision of the
two eyes.
In
the treatment of functional eye troubles this relationship between
relaxation and memory is of great practical importance. The
sensations of the eye and of the mind supply very little information
as to the strain to which both are being subjected, those who strain
most often suffering the least discomfort; but by means of his
ability to remember black the patient can always know whether he is
straining or not, and is able, therefore, to avoid the conditions
that produce strain. Whatever method of improving his sight the
patient is using, he is advised to carry with him constantly the
memory of a small area of black, such as a period, so that he may
recognize and avoid the conditions that produce strain, and in
some cases patients have obtained a complete cure in a very short
time by this means alone. One advantage of the method is that it does
not require a test card, for at any hour of the day or night,
whatever the patient may be doing, he can always place himself in the
conditions favorable to the perfect memory of a period.
The
condition of mind in which a black period can be remembered cannot be
attained by any sort of effort. The memory is not the cause of the
relaxation, but must be preceded by it. It is obtained only
during moments of relaxation, and retained only as long as the causes
of strain are avoided; but how this is accomplished cannot be fully
explained, just as many other psychological phenomena cannot be
explained. We only know that under certain conditions that might
be called favorable a degree of relaxation sufficient for the memory
of a black period is possible, and that, by persistently seeking
these conditions, the patient becomes able to increase the
degree of the relaxation and prolong its duration, and finally
becomes able to retain it under unfavorable conditions.
For
most patients palming provides the most favorable conditions for
the memory of black. When the
strain
to see is lessened by the exclusion of the light, the patient usually
becomes able to remember a black object for a few seconds or longer,
and this period of relaxation can be prolonged in one of two ways.
Either the patient can open his eyes and look at a black object by
central fixation at the distance at which it can be seen best, and at
which the eyes are, therefore, most relaxed, or he can shift
mentally from one black object to another, or from one part of a
black object to another. By these means, and perhaps also through
other influences that are not clearly understood, most patients
become able, sooner or later, to remember black for an indefinite
length of time with their eyes closed and covered.
With
the eyes open and looking at a blank surface without trying
consciously to see, the unconscious strain is lessened so that the
patient becomes able to remember a black period, and all errors of
refraction, as demonstrated by the retinoscope, are corrected.
This result has been found to be invariable, and so long as the
surface remains blank and the patient does not begin to remember or
imagine things seen imperfectly, the memory and the vision may be
retained. But if, with the improved vision, details upon the surface
begin to come out, or if the patient begins to think of the test
card, which he has seen imperfectly, the strain to see will return
and the period will be lost.
When
looking at a surface on which there is nothing particular to see,
distance makes no difference to the memory, because the patient can
always look at such a surface, no matter where it is, without
straining to see it. When looking at letters, or other details,
however, the memory is best at the point at which the patient's sight
is best, because at that point the eyes and mind are more relaxed
than when the same letters or objects are regarded at distances
at which the vision is not so good. By practicing central
fixation at the most favorable distance, therefore, and using
any other means of improving the vision which are found effectual,
the memory of the period may be improved, in some cases, very
rapidly.
If
the relaxation gained under these favorable conditions is perfect,
the patient will be able to retain it when the mind is conscious of
the impressions of sight at unfavorable distances. Such cases
are, however, very rare. Usually the degree of relaxation gained
is markedly imperfect, and is, therefore, lost to a greater or
less degree when the conditions are unfavorable, as when letters
or objects are being regarded at unfavorable distances. So
disturbing are the impressions of sight under these circumstances,
that just as soon as details begin to come out at distances at which
they have not previously been seen, the patient usually loses his
relaxation, and with it the memory of the period. In fact, the strain
to see may even return before he has had time to become conscious of
the image on his retina, as the following case strikingly
illustrates:
A
woman of fifty-five who had myopia of fifteen diopters, complicated
with other conditions which made it impossible for her to see the big
C at more than one foot, or to go about, either in her house or on
the street, without an attendant, became able, when she looked at a
green wall without trying to see it, to remember a perfectly black
period and to see a small area of the wall-paper at the distance as
well as she could at the near-point. When she had come close to the
wall, she was asked to put her hand on the door-knob, which she did
without hesitation. "But I don't see the knob," she
hastened to explain. As a matter of fact she had seen it long enough
to put her hand on it; but as soon as the idea of seeing it was
suggested to her she lost the memory of the period, and with it
her improved vision, and when she again tried to find the knob she
could not do so.
When
a period is remembered perfectly while a letter on the Snellen test
card is being regarded, the letter improves, with or without the
consciousness of the patient; because it is impossible to strain
and relax at the same time, and if one relaxes sufficiently to
remember the period, one must also relax sufficiently to see the
letter, consciously or unconsciously. Letters on either side of the
one regarded, or on the lines above and below it, also improve. When
the patient is conscious of seeing the letters, this is very
distracting, and usually causes him, at first, to forget the period;
while with some patients, as already noted the strain may return even
before the letters are consciously recognized.
Thus
patients find themselves on the horns of a dilemma. The relaxation
indicated by the memory of a period improves their sight, and the
things they see with this improved vision cause them to lose their
relaxation and their memory. It is very remarkable to me how the
difficulty is ever overcome, but some patients are able to do it in
five minutes or half an hour. With others the process is long and
tedious.
There
are various ways of helping patients to deal with this situation. One
is to direct them to remember the period while looking a little
to one side of the test card, say a foot or more; then to look a
little nearer to it, and finally to look between the lines. In this
way they may become able to see the letters in the eccentric field
without losing the period; and when they can do this they may become
able to go a step farther, and look directly at a letter without
losing control of their memory. If they cannot do it, they are told
to look at only one part of a letter - usually the bottom - or to see
or imagine the period as part of the letter, while noting that the
rest of the letter is less black and less distinct than the part
directly regarded- When they can do this they become able to remember
the period better than when the letter is seen all alike. If the
letter is seen all alike, the perfect memory of the period is always
lost. The next step is to ask the patient to note whether the bottom
of the letter is straight, curved, or open, without losing the period
on the bottom. When he can do this, he is asked to do the same with
the sides and top of the letter, still holding the period on the
bottom. Usually when the parts can be observed separately in this
way, the whole letter can be seen without losing the memory of the
period; but it occasionally happens that this is not the case, and
further practice is needed before the patient can become conscious of
all sides of the letter at once without losing the period. This may
require moments, hours, days, or months. In one case the following
method succeeded:
The
patient, a man with fifteen diopters of myopia, was so much disturbed
by what he saw when his vision had been improved by the memory of a
period that he was directed to look away from the Snellen test card,
or whatever object he was regarding, when he found the letters or
other details coming out; and for about a week he went around
persistently dodging his improved sight. As his memory improved,
it became more and more difficult for him to do this, and at the end
of the week it was impossible. When he looked at the bottom line
at a distance of twenty feet he remembered the period perfectly,
and when asked if he could see the letters, he replied:
"I
cannot help but see them."
Some
patients retard their recovery by decorating the scenery with periods
as they go about during the day, instead of simply remembering a
period in their minds. This does them no good, but is, on the
contrary, a cause of strain. The period can be imagined
perfectly and with benefit as forming part of a black letter on the
test card, because this merely means imagining that one sees one part
of the black letter best; but it cannot be imagined perfectly on any
surface which is not black, and to attempt to imagine it on such
surfaces defeats the end in view.
The
smaller the area of black which the patient is able to remember, the
greater is the degree of relaxation indicated; but some patients find
it easier, at first, to remember a somewhat larger area, such as one
of the letters on the Snellen test card with one part blacker than
the rest. They may begin with the big C, then proceed to the smaller
letters, and finally get to a period. It is then found that this
small area is remembered more easily than the larger ones, and that
its black is more intense. Instead of a period, some patients find it
easier to remember a colon, with one period blacker than the other,
or a collection of periods, with one blacker than all the others, or
the dot over an i or j. Others, again, prefer a comma to a period. In
the beginning most patients find it helpful to shift consciously from
one of these black areas to another, or from one part of such an area
to another, and to realize the swing, or pulsation, produced by such
shifting (see Chapter XV); but when the memory becomes perfect, one
object may be held continuously, without conscious shifting,
while the swing is realized only when attention is directed to the
matter.
Although
black is, as a rule, the best color to remember, some patients
are bored or depressed by it, and prefer to remember white or some
other color. A familiar object, or one with pleasant associations,
is often easier to remember than one which has no particular
interest. One patient was cured by the memory of a yellow buttercup,
and another was able to remember the opal of her ring when she could
not remember a period. Whatever the patient finds easiest to remember
is the best to remember, because the memory can never be perfect
unless it is easy.
When
the memory of the period becomes habitual, it is not only not a
burden, but is a great help to other mental processes. The mind, when
it remembers one thing better than all other things, possesses
central fixation, and its efficiency is thereby increased, just as
the efficiency of the eye is increased by central fixation. In other
words, the mind attains its greatest efficiency when it is at rest,
and it is never at rest unless one thing is remembered better than
all other things. When the mind is in such a condition that a period
is remembered perfectly, the memory for other things is improved.
A
high-school girl reports that when she was unable to remember the
answer to a question in an examination, she remembered the
period, and the answer came to her. When I cannot remember the name
of a patient, I remember a period - and, behold, I have it! A
musician who had perfect sight and could remember a period
perfectly, had a perfect memory for music; but a musician with
imperfect sight who could not remember a period could play nothing
without his notes, only gaining that power when his sight and
visual memory had become normal. In some exceptional cases, the
strain to see letters on the Snellen test card has been so terrific
that patients have said that they not only could not remember a
period while they were looking at them, but could not remember even
their own names.
Patients
may measure the accuracy of their memory of the period, not only by
comparing it with the sight, but by the following tests: When the
memory of the period is perfect it is instantaneous. If a few seconds
or longer are necessary to obtain the memory, it is never
perfect.
A
perfect memory is not only instantaneous, but continuous. When the
period is remembered perfectly perfect sight comes
instantaneously. If good vision is obtained only after a second or
two, it can always be demonstrated that the memory of the period is
imperfect and the sight also.
The
memory of a period is a test of relaxation. It is the evidence by
which the patient knows that his eyes and mind are at rest. It may be
compared to the steam-gauge of an engine, which has nothing to do
with the machinery, but is of great importance in giving information
as to the ability of the mechanism to do its work. When the period is
black one knows that the engine of the eye is in good working order.
When the period fades, or is lost, one knows that it is out of order,
until a cure is effected. Then one does not need a period, or any
other aid to vision, just as the engineer does not need a steam-gauge
when the engine is going properly. One patient who had gained
telescopic and microscopic vision by the methods presented in this
book said, in answer to an inquiry from some one interested in
investigating the treatment of errors of refraction without glasses,
that he had not only done nothing to prevent a relapse, but had
even forgotten how he was cured. The reply was unsatisfactory to the
inquirer, but is quoted to illustrate the fact that when a patient is
cured he does not need to do anything consciously in order to stay
cured, although the treatment can always be continued with benefit,
since even supernormal vision can be improved.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XIV
IMAGINATION AS AN AID TO VISION
We
see very largely with the mind, and only partly with the eyes. The
phenomena of vision depend upon the mind's interpretation of the
impression upon the retina. What we see is not that impression, but
our own interpretation of it. Our impressions of size, color, form
and location can be demonstrated to depend upon the interpretation by
the mind of the retinal picture. The moon looks smaller at the zenith
than it does at the horizon, though the optical angle is the same and
the impression on the retina may be the same, because at the horizon
the mind unconsciously compares the picture with the pictures of
surrounding objects, while at the zenith there is nothing to compare
it with. The figure of a man on a high building, or on the topmast of
a vessel, looks small to the landsman; but to the sailor it appears
to be of ordinary size, because he is accustomed to seeing the human
figure in such positions.
Persons
with normal vision use their memory, or imagination, as an aid to
sight; and when the sight is imperfect it can be demonstrated, not
only that the eye itself is at fault, but that the memory and
imagination are impaired, so that the mind adds imperfections
to the imperfect retinal image. No two persons with normal sight will
get the same visual impressions from the same object; for their
interpretations of the retinal picture will differ as much as
their individualities differ, and when the sight is imperfect the
interpretation is far more variable. It reflects, in fact, the loss
of mental control which is responsible for the error of refraction.
When the eye is out of focus, in short, the mind is also out of
focus.
According
to the accepted view most of the abnormalities of vision
produced when there is an error of refraction in the eye are
sufficiently accounted for
by
the existence of that error. Some are supposed to be due to diseases
of the brain or retina. Multiple images are attributed to
astigmatism, though only two can be legitimately accounted for in
this way, while some patients state that they see half a dozen or
more, and many persons with astigmatism do not see any. It can easily
be demonstrated, however, that the inaccuracy of the focus accounts
for only a small part of these results; and since they can all be
corrected in a few seconds through the correction, by relaxation, of
the error of refraction, it is evident that they cannot be due to any
organic disease.
If
we compare the picture on the glass screen of the camera when the
camera is out of focus with the visual impressions of the mind when
the eye is out of focus, there will be found to be a great difference
between them. When the camera is out of focus it turns black into
grey, and blurs the outlines of the picture; but it produces these
results uniformly and constantly. On the screen of the camera an
imperfect picture of a black letter would be equally imperfect in all
parts, and the same adjustment of the focus would always produce the
same picture. But when the eye is out of focus the imperfect picture
which the patient imagines that he sees is always changing, whether
the focus changes or not. There will be more grey on one part
than on another, and both the shade and the position of the grey may
vary within wide limits in a very short space of time. One part of
the letter may appear grey and the rest black. Certain outlines may
be seen better than others, the vertical lines, perhaps, appearing
black and the diagonal grey, and vice versa. Again, the black may be
changed into brown, yellow, green, or even red, transmutations
impossible to the camera. Or there may be spots of color, or of
black, on the grey, or on the white openings. There may also be spots
of white, or of color, on the black.
When
the camera is out of focus the picture which it produces of any
object is always slightly larger than the image produced when the
focus is correct; but when the eye is out of focus the picture which
the mind sees may be either larger or smaller than it normally would
be. To one patient the big C at ten feet appeared smaller than at
either twenty feet or four inches. To some it appears larger than it
actually is at twenty feet, and to others it seems smaller.
When
the human eye is out of focus the form of the objects regarded by the
patient frequently appears to be distorted, while their location may
also appear to change. The image may be doubled, tripled, or still
further multiplied, and while one object, or part of an object may be
multiplied other objects or parts of objects in the field of vision
may remain single. The location of these multiple images is
sometimes constant and at others subject to continual
change. Nothing like this could happen when the camera is out of
focus.
If
two cameras are out of focus to the same degree, they will take two
imperfect pictures exactly alike. If two eyes are out of focus to the
same degree, similar impressions will be made upon the retina of
each; but the impressions made upon the mind may be totally unlike,
whether the eyes belong to the same person or to different persons.
If the normal eye looks at an object through glasses that change its
refraction, the greyness and blurring produced are uniform and
constant; but when the eye has an error of refraction equivalent to
that produced by the glasses, these phenomena are nonuniform and
variable.
It
is fundamental that the patient should understand that these
aberrations of vision - which are treated more fully in a later
chapter - are illusions, and not due to a fault of the eyes. When he
knows that a thing is an illusion he is less likely to see it again.
When he becomes convinced that what he sees is imaginary it helps to
bring the imagination under control; and since a perfect imagination
is impossible without perfect relaxation, a perfect imagination not
only corrects the false interpretation of the retinal image, but
corrects the error of refraction.
Imagination
is closely allied to memory, although distinct from it. Imagination
depends upon the memory, because a thing can be imagined only as
well as it can be remembered. You cannot imagine a sunset unless you
have seen one; and if you attempt to imagine a blue sun, which you
have never seen, you will become myopic, as indicated by simultaneous
retinoscopy. Neither imagination nor memory can be perfect
unless the mind is perfectly relaxed.
Therefore
when the imagination and memory are perfect, the sight is perfect.
Imagination, memory and sight are, in fact, coincident. When one is
perfect, all are perfect, and when one is imperfect, all are
imperfect. If you imagine a letter perfectly, you will see the letter
and other letters in its neighborhood will come out more
distinctly, because it is impossible for you to relax and imagine you
see a perfect letter and at the same time strain and actually see an
imperfect one. If you imagine a perfect period on the bottom of
a letter, you will see the letter perfectly, because you cannot take
the mental picture of a perfect period and put it on an imperfect
letter. It is possible, however, as pointed out in the preceding
chapter, for sight to be unconscious. In some cases patients may
imagine the period perfectly, as demonstrated by the retinoscope,
without being conscious of seeing the letter; and it is often some
time before they are able to be conscious of it without losing the
period.
When
one treats patients who are willing to believe that the letters can
be imagined, and who are content to imagine without trying to
see, or compare what they see with what they imagine, which always
brings back the strain, very remarkable results are sometimes
obtained by the aid of the imagination. Some patients at once become
able to read all the letters on the bottom line of the test card
after they become able to imagine that they see one letter
perfectly black and distinct. The majority, however, are so
distracted by what they see when their vision has been improved by
their imagination that they lose the latter. It is one thing to be
able to imagine perfect sight of a letter, and another to be able to
see the letter and other letters without losing control of the
imagination.
In
myopia the following method is often successful:
First
look at a letter at the point at which it is seen best. Then close
the eyes and remember it. Repeat until the memory is almost as good
as the sight at the nearpoint. With the test card at a distance of
twenty feet, look at a blank surface a foot or more to one side of
it, and again remember the letter. Do the same at six inches and at
three inches. At the last point note the appearance of the letters on
the card - that is, in the eccentric field. If the memory is still
perfect, they will appear to be a dim black, not grey, and those
nearest the point of fixation will appear blacker than those more
distant. Gradually reduce the distance between the point of fixation
and the letter until able to look straight at it and imagine that it
is seen as well as it is remembered. Occasionally it is well during
the practice to close and cover the eyes and remember the letter, or
a period, perfectly black. The rest and mental control gained in this
way are a help in gaining control when one looks at the test card.
Patients
who succeed with this method are not conscious while imagining a
perfect letter, of seeing, at the same time, an imperfect one, and
are not distracted when their vision is improved by their
imagination. Many patients can remember perfectly with
their eyes closed, or when they are looking at a place where they
cannot see the letter; but just as soon as they look at it they begin
to strain and lose control of their memory. Therefore, as the
imagination depends upon the memory, they cannot imagine that
they see the letter. In such cases it has been my custom to proceed
somewhat in the manner described in the preceding chapter. I begin by
saying to the patient:
"Can
you imagine a black period on the bottom of this letter, and at the
same time, while imagining the period perfectly, are you able to
imagine that you see the letter?"
Sometimes
they are able to do this, but usually they are not. In that case they
are asked to imagine part of the letter, usually the bottom. When
they have become able to imagine this part straight, curved, or open,
as the case may be, they become able to imagine the sides and top,
while still holding the period on the bottom. But even after they
have done this, they may still not be able to imagine the whole
letter without losing the period. One may have to coax them along by
bringing the card up a little closer, then moving it farther away;
for when looking at a surface where there is anything to see, the
imagination improves in proportion as one approaches the point where
the sight is best, because at that point the eyes are most relaxed.
When there is nothing particular to see, the distance makes no
difference, because no effort is being made to see.
To
encourage patients to imagine they see the letter it seems helpful to
keep saying to them over and over again:
"Of
course you do not see the letter. I am not asking you to see it.
I am just asking you to imagine that you see it perfectly black and
perfectly distinct."
When
patients become able to see a known letter by the aid of their
imagination, they become able to apply the same method to an unknown
letter; for just as soon as any part of a letter, such as an area
equal to a period, can be imagined to be perfectly black, the whole
letter is seen to be black, although the visual perception of this
fact may not, at first, last long enough for the patient to become
conscious of it.
In
trying to distinguish unknown letters, the patient discovers that it
is impossible to imagine perfectly unless one imagines the truth; for
if a letter, or any part of a letter, is imagined to be other than it
is, the mental picture is foggy and inconstant, just like a letter
which is seen imperfectly.
The
ways in which the imagination can be interfered with are very
numerous. There is one way of imagining perfectly and an
infinite number of ways of imagining imperfectly. The right way is
easy. The mental picture of the thing imagined comes as quick as
thought, and can be held more or less continuously. The wrong
way is difficult. The picture comes slowly, and is both variable and
discontinuous. This can be demonstrated to the patient by asking him
first to imagine or remember a black letter as perfectly as
possible with the eyes closed, and then to imagine the same letter
imperfectly. The first he can usually do easily; but it will be found
very difficult to imagine a black letter with clear outlines to
be grey, with fuzzy edges and clouded openings, and impossible to
form a mental picture of it that will remain constant for an
appreciable length of time. The letter will vary in color, shape and
location in the visual field, precisely as a letter does when it is
seen imperfectly; and just as the strain of imperfect sight
produces discomfort and pain, the effort to imagine imperfectly will
sometimes produce pain. The more nearly perfect the mental picture of
the letter, on the contrary, the more easily and quickly it comes and
the more constant it is.
Some
very dramatic cures have been effected by means of the-imagination.
One patient, a physician, who had worn glasses for forty years and
who could not without them see the big C at twenty feet, was cured in
fifteen minutes simply by imagining that he saw the letters black.
When asked to describe the big C with unaided vision he said it
looked grey to him, and that the opening was obscured by a grey cloud
to such an extent that he had to guess that it had an opening. He was
told that the letter was black, perfectly black, and that the opening
was perfectly white, with no grey cloud; and the card was brought
close to him so that he could see that this was so. When he again
regarded the letter at the distance, he remembered its blackness so
vividly that he was able to imagine that he saw it just as black as
he had seen it at the near-point, with the opening perfectly white;
and therefore he saw the letter on the card perfectly black and
distinct. In the same way he became able to read the seventy line;
and so he went down the card, until in about five minutes he became
able to read at twenty feet the line which the normal eye is supposed
to read at ten feet. Next diamond type was given to him to read. The
letters appeared grey to him, and he could not read them. His
attention was called to the fact that the letters were really black,
and immediately he imagined that he saw them black and became able to
read them at ten inches.
The
explanation of this remarkable occurrence is simply relaxation. All
the nerves of the patient's body were relaxed when he imagined that
he saw the letters black, and when he became conscious of seeing
the letters on the card, he still retained control of his
imagination. Therefore he did not begin to strain again, and actually
saw the letters as black as he imagined them.
The
patient not only had no relapse, but continued to improve. About a
year later I visited him in his office and asked him how he was
getting on. He replied that his sight was perfect, both for distance
and the near-point. He could see the motor cars on the other side of
the Hudson River and the people in them, and he could read the names
of boats on the river which other people could make out only with a
telescope. At the same time he had no difficulty in reading the
newspapers, and to prove the latter part of this statement, he picked
up a newspaper and read a few sentences aloud. I was astonished, and
asked him how he did it.
"I
did what you told me to do," he said.
"What
did I tell you to do?" I asked.
"You
told me to read the Snellen test card every day, which I have done,
and to read fine print every day in a dim light, which I have also
done."
Another
patient, who had a high degree of myopia complicated with atrophy of
the optic nerve, and who had been discouraged by many physicians, was
benefited so wonderfully and rapidly by the aid of his imagination
that one day while in the office he lost control of himself
completely, and raising a test card which he held in his hand, he
threw it across the room.
"It
is too good to be true," he exclaimed; "I cannot believe
it. The possibility of being cured and the fear of disappointment are
more than I can stand."
He
was calmed down with some difficulty and encouraged to continue.
Later he became able to read the small letters on the test card with
normal vision. He was then given fine print to read. When he looked
at the diamond type, he at once said that it was impossible for him
to read it. However, he was told to follow the same procedure that
had benefited his distance sight. That is, he was to imagine a
period on one part of the small letters while holding the type at six
inches. After testing his memory of the period a number of times, he
became able to imagine he saw a period perfectly black on one of the
small letters. Then he lost control of his nerves again, and on being
asked, "What is the trouble ?" he said:
"I
am beginning to read the fine print, and I am so overwhelmed that I
lose my self-control."
In
another case, that of a woman with high myopia complicated with
incipient cataract, the vision improved in a few days from 3/200
to 20/50. Instead of going gradually down the card, a jump was made
from the fifty line to the ten line. The card was brought up close to
her, and she was asked to look at the letter O at three inches, the
distance at which she saw it best, to imagine that she saw a period
on the bottom of it and that the bottom was the blackest part. When
she was able to do this at the near-point, the distance was gradually
increased until she became able to see the O at three feet. Then I
placed the card at ten feet and she exclaimed:
"Oh,
doctor, it is impossible! The letter is too small. It is too great a
thing for me to do. Let me try a larger letter first."
Nevertheless
she became able in fifteen minutes to read the small O on the ten
line at twenty feet.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XV
SHIFTING AND SWINGING
When
the eye with normal vision regards a letter either at the near-point
or at the distance, the letter may appear to pulsate, or to move in
various directions, from side to side, up and down, or obliquely.
When it looks from one letter to another on the Snellen test card, or
from one side of a letter to another, not only the letter, but the
whole line of letters and the whole card, may appear to move from
side to side. This apparent movement is due to the shifting of the
eye, and is always in a direction contrary to its movement. If one
looks at the top of a letter, the letter is below the line of vision,
and, therefore, appears to move downward. If one looks at the bottom,
the letter is above the line of vision and appears to move upward. If
one looks to the left of the letter, it is to the right of the line
of vision and appears to move to the right. If one looks to the
right, it is to the left of the line of vision and appears to move to
the left.
Persons
with normal vision are rarely conscious of this illusion, and may
have difficulty in demonstrating it; but in every case that has
come under my observation they have always become able, in a longer
or shorter time, to do so. When the sight is imperfect the letters
may remain stationary, or even move in the same direction as the eye.
It
is impossible for the eye to fix a point longer than a fraction of a
second. If it tries to do so, it begins to strain and the vision is
lowered. This can readily be demonstrated by trying to hold one part
of a letter for an appreciable length of time. No matter how good the
sight, it will begin to blur, or even disappear, very quickly, and
sometimes the effort to hold it will produce pain. In the case of a
few exceptional people a point may appear to be held for a
considerable length of time; the subjects themselves may think that
they are holding it; but this is only because the eye shifts
unconsciously, the movements being so rapid that objects seem to be
seen all alike simultaneously.
The
shifting of the eye with normal vision is usually not conspicuous,
but by direct examination with the ophthalmoscope it can always be
demonstrated. If one eye is examined with this instrument while the
other is regarding a small area straight ahead, the eye being
examined, which follows the movements of the other, is seen to move
in various directions, from side to side, up and down in an orbit
which is usually variable. If the vision is normal these movements
are extremely rapid and unaccompanied by any appearance of effort.
The shifting of the eye with imperfect sight, on the contrary, is
slower, its excursions are wider, and the movements are jerky and
made with apparent effort.
It
can also be demonstrated that the eye is capable of shifting with a
rapidity which the ophthalmoscope cannot measure. The normal eye can
read fourteen letters on the bottom line of a Snellen test card, at a
distance of ten or fifteen feet, in a dim light, so rapidly that they
seem to be seen all at once. Yet it can be demonstrated that in order
to recognize the letters under these conditions it is necessary to
make about four shifts to each letter. At the near-point,:even though
one part of the letter is seen best, the rest may be seen well enough
to be recognized; but at the distance it is impossible to
recognize the letters unless one shifts from the top to the
bottom and from side to side. One must also shift from one letter to
another, making about seventy shifts in a fraction of a second.
A
line of small letters on the Snellen test card may be less than a
foot long by a quarter of an inch in height; and if it requires
seventy shifts to a fraction of a second to see it apparently
all at once, it must require many thousands to see an area of the
size of the screen of a moving picture, with all its detail of
people, animals, houses, or trees, while to see sixteen such areas to
a second, as is done in viewing moving pictures, must require a
rapidity of shifting that can scarcely be realized. Yet it is
admitted that the present rate of taking and projecting moving
pictures is too slow. The results would be more satisfactory,
authorities say, if the rate were raised to twenty, twenty-two, or
twenty-four a second.
The
human eye and mind are not only capable of this rapidity of action,
and that without effort or strain, but it is only when the eye is
able to shift thus rapidly that eye and mind are at rest, and
the efficiency of both at their maximum. It is true that every
motion of the eye produces an error of refraction; but when the
movement is short, this is very slight, and usually the shifts are so
rapid that the error does not last long enough to be detected by the
retinoscope, its existence being demonstrable only by reducing
the rapidity of the movements to less than four or five a
second. The period during which the eye is at rest is much longer
than that during which an error of refraction is produced.
Hence, when the eye shifts normally no error of refraction is
manifest. The more rapid the unconscious shifting of the eye,
the better the vision; but if one tries to be conscious of a too
rapid shift, a strain will be produced.
Perfect
sight is impossible without continual shifting, and such
shifting is a striking illustration of the mental control necessary
for normal vision. It requires perfect mental control to think
of thousands of things in a fraction of a second; and each point of
fixation has to be thought of separately, because it is impossible to
think of two things, or of two parts of one thing, perfectly at the
same time. The eye with imperfect sight tries to accomplish the
impossible by looking fixedly at one point for an appreciable
length of time; that is, by staring. When it looks at a strange
letter and does not see it, it keeps on looking at it in an effort to
see it better. Such efforts always fail, and are an important factor
in the production of imperfect sight.
One
of the best methods of improving the sight, therefore, is to imitate
consciously the unconscious shifting of normal vision and to realize
the apparent motion produced by such shifting. Whether one has
imperfect or normal sight, conscious shifting and swinging are a
great help and advantage to the eye; for not only may imperfect sight
be improved in this way, but normal sight may be improved also. When
the sight is imperfect, shifting, if done properly, rests the eye as
much as palming, and always lessens or corrects the error of
refraction.
The
eye with- normal sight never attempts to hold a point more than a
fraction of a second, and when it shifts, as explained in the chapter
on "Central Fixation," it always sees the previous point of
fixation worse. When it ceases to shift rapidly and to see the
point shifted from worse, the sight ceases to be normal, the swing
being either prevented or lengthened, or (occasionally) reversed.
These facts are the keynote of the treatment by shifting.
In
order to see the previous point of fixation worse, the eye with
imperfect sight has to look farther away from it than does the eye
with normal sight. If it shifts only a quarter of an inch, for
instance, it may see the previous point of fixation as well as or
better than before; and instead of being rested by such a shift, its
strain will be increased, there will be no swing, and the vision will
be lowered. At a couple of inches it may be able to let go of the
first point; and if neither point is held more than a fraction
of a second, it will be rested by such a shift and the illusion of
swinging may be produced. The shorter the shift the greater the
benefit; but even a very long shift - as much as three feet or more -
is a help to those who cannot accomplish a shorter one. When the
patient is capable of a short shift, on the contrary, the long shift
lowers the vision. The swing is an evidence that the shifting is
being done properly, and when it occurs the vision is always
improved. It is possible to shift without improvement; but it is
impossible to produce the illusion of a swing without improvement,
and when this can be done with a long shift, the movement can
gradually be shortened until the patient can shift from the top to
the bottom of the smallest letter, on the Snellen test card or
elsewhere, and maintain the swing. Later he may become able to be
conscious of the swinging of the letters without conscious shifting.
No
matter how imperfect the sight, it is always possible to shift and
produce a swing, so long as the previous point of fixation is seen
worse. Even diplopia and polyopia(1) do not prevent swinging with
some improvement of vision. Usually the eye with imperfect vision is
able to shift from one side of the card to the other, or from a point
above the card to a point below it, and observe that in the first
case the card appears to move from side to side, while in the second
it appears to move up and down.
When
patients are suffering from high degrees of eccentric fixation, it
may be necessary, in order to help them to see worse when they shift,
to use some of the methods described in the chapter on "Central
Fixation." Usually, however, patients who cannot see worse when
they shift at the distance can do it readily at the near-point, as
the sight is best at that point, not only in myopia, but often in
hypermetropia as well. When the swing can be produced at the
near point, the distance can be gradually increased until the
same thing can be done at twenty feet.
After
resting the eyes by closing or palming, shifting and swinging
are often more successful. By this method of alternately resting the
eyes and then shifting, persons with very imperfect sight have
sometimes obtained a temporary or permanent cure in a few weeks.
Shifting
may be done slowly or rapidly, according to the state of the vision.
At the beginning the patient will be likely to strain if he shifts
too rapidly; and then the point shifted from will not be seen worse,
and there will be no swing. As improvement is made, the speed can be
increased. It is usually impossible, however, to realize the swing if
the shifting is more rapid than two or three times a second.
A
mental picture of a letter can, as a rule, be made to swing precisely
as can a letter on the test card. Occasionally one meets a patient
with whom the reverse is true; but for most patients the mental swing
is easier at first than visual swinging; and when they become able to
swing in this way, it becomes easier for them to swing the
letters on the test card. By alternating mental with visual swinging
and shifting, rapid progress is sometimes made. As relaxation becomes
more perfect, the mental swing can be shortened, until it becomes
possible to conceive and swing a letter the size of a period in a
newspaper. This is easier, when it can be done, than swinging a
larger letter, and many patients have derived great benefit from it.
All
persons, no matter how great their error of refraction, when they
shift and swing successfully, correct it partially or completely, as
demonstrated by the retinoscope, for at least a fraction of a
second. This time may be so short that the patient is not
conscious of improved vision; but it is possible for him to imagine
it, and then it becomes easier to maintain the relaxation long enough
to be conscious of the improved sight. For instance, the patient,
after looking away from the card, may look back to the big C, and for
a fraction of a second the error of refraction may be lessened or
corrected, as demonstrated by the retinoscope. Yet he may not be
conscious of improved vision. By imagining that the C is seen better,
however, the moment of relaxation may be sufficiently prolonged to be
realized.
When
swinging, either mental or visual, is successful, the patient may
become conscious of a feeling of relaxation which is manifested as a
sensation of universal swinging. This sensation communicates itself
to any object of which the patient is conscious. The motion may
be imagined in any part of the body to which the attention is
directed. It may be communicated to the chair in which the patient is
sitting, or to any object in the room, or elsewhere, which is
remembered. The building, the city, the whole world, in fact, may
appear to be swinging. When the patient becomes conscious of this
universal swinging, he loses the memory of the object with which
it started; but so long as he is able to maintain the movement in a
direction contrary to the original movement of the eyes, or the
movement imagined by the mind, relaxation is maintained. If the
direction is changed, however, strain results. To imagine the
universal swing with the eyes closed is easy, and some patients soon
become able to do it with the eyes open. Later the feeling of
relaxation which accompanies the swing may be realized without
consciousness of the latter; but the swing can always be
produced when the patient thinks of it.
There
is but one cause of failure to produce a swing, and that is strain
Some people try to make the letters swing by effort. Such
efforts always fail. The eyes and mind do not swing the letters; they
swing of themselves. The eye can shift voluntarily. This is a
muscular act resulting from a motor impulse. But the swing comes of
its own accord when the shifting is normal. It does not produce
relaxation, but is an evidence of it; and while of no value in itself
is, like the period, very valuable as an indication that relaxation
is being maintained.
The
following methods of shifting have been found useful in various
cases:
No.
l -
|
(a)
|
Regard
a letter.
|
|
(b)
|
Shift
to a letter on the same line far enough away so that the first is
seen worse.
|
|
(c)
|
Look
back at No. l and see No. 2 worse.
|
|
(d)
|
Look
at the letters alternately for a few seconds, seeing worse the
one not regarded.
|
When
successful, both letters improve and appear to move from side to side
in a direction opposite to the movement of the eye.
No.
2 -
|
(a)
|
Look
at a large letter.
|
|
(b)
|
Look
at a smaller one a long distance away from it. The large one is
then seen worse.
|
|
(c)
|
Look
back and see it better.
|
|
(d)
|
Repeat
half a dozen times.
|
When
successful, both letters improve, and the card appears to move up and
down.
No.
3 -
Shifting
by the above methods enables the patient to see one letter on a line
better than the other letters, and, usually, to distinguish it in
flashes. In order to see the letter continuously it is necessary
to
become able to shift from the top to the bottom, or from the bottom
to the top, seeing worse the part not directly regarded, and
producing the illusion of a vertical swing.
|
(a)
|
Look
at a point far enough above the top of the letter to see the
bottom, or the whole letter worse.
|
|
(b)
|
Look
at a point far enough below the bottom to see the top, or the
whole letter, worse.
|
|
(c)
|
Repeat
half a dozen times.
|
If
successful, the letter will appear to move up and down, and the
vision will improve. The shift can then be shortened until it becomes
possible to shift between the top and the bottom of the letter and
maintain the swing. The letter is now seen continuously. If the
method fails, rest the eyes, palm, and try again.
One
may also practice by shifting from one side of the letter to a point
beyond the other side, or from one corner to a point beyond the other
corner.
No.
4 -
|
(a)
|
Regard
a letter at the distance at which it is seen best. In myopia this
will be at the near-point, a foot or less from the face. Shift
from the top to the bottom until able to see each worse
alternately, when the letter will appear blacker than before, and
an illusion of swinging will be produced.
|
|
(b)
|
Now
close the eyes, and shift from the top to the bottom of the
letter mentally.
|
|
(c)
|
Regard
a blank wall with the eyes open, and do the same. Compare the
ability to shift and swing mentally with the ability to do the
same visually at the near-point.
|
|
(d)
|
Then
regard the letter at the distance, and shift from the top to the
bottom. If successful, the letter will improve, and an illusion
of swinging will be produced.
|
No.
5 -
Some
patients, particularly children, are able to see better when one
points to the letters. In other cases this is a distraction. When the
method is found successful one can proceed as follows:
|
(a)
|
Place
the tip of the finger three or four inches below the letter. Let
the patient regard the letter, and shift to the tip of the
finger, seeing the letter worse.
|
|
(b)
|
Reduce
the distance between the finger and the letter, first to two or
three inches, then to one or two, and finally to half an inch,
proceeding each time as in (a).
|
If
successful, the patient will become able to look from the top to the
bottom of the letter, seeing each worse alternately, and producing
the illusion of swinging. It will then be possible to see the letter
continuously.
No.
6 -
When
the vision is imperfect it often happens that, when the patient looks
at a small letter, some of the larger letters on the upper lines, or
the big C at the top, look blacker than the letter regarded. This
makes it impossible to see the smaller letters perfectly. To correct
this eccentric fixation regard the letter which is seen best, and
shift to the smaller letter. If successful, the small letter, after a
few movements, will appear blacker than the larger one. If not
successful after a few trials, rest the eyes by closing and palming,
and try again. One may also shift from the large letter to a point
some distance below the small letter, gradually approaching the
latter as the vision improves.
No.
7 -
Shifting
from a card at three or five feet to one at ten or twenty feet often
proves helpful, as the unconscious memory of the letter seen at the
near-point helps to bring out the one at the distance.
Different
people will find these various methods of shifting more or less
satisfactory. If any method
does
not succeed, it should be abandoned after one or two trials and
something else tried. It is a mistake to continue the practice
of any method which does not yield prompt results. The cause of the
failure is strain, and it does no good to continue the strain.
When
it is not possible to practice with the Snellen test card, other
objects may be utilized. One can shift, for instance, from one window
of a distant building to another, or from one part of a window to
another part of the same window, from one auto to another, or from
one part of an auto to another part, producing, in each case, the
illusion that the objects are moving in a direction contrary to the
movement of the eye.
When
talking to people, one can shift from one person to another, or from
one part of the face to another part. When reading a book, or
newspaper, one can shift consciously from one word or letter to
another, or from one part of a letter to another.
Shifting
and swinging, as they give the patient something definite to do, are
often more successful than other methods of obtaining relaxation, and
in some cases remarkable results have been obtained simply by
demonstrating to the patient that staring lowers the vision and
shifting improves it. One patient, a girl of sixteen with progressive
myopia, obtained very prompt relief by shifting. She came to the
office wearing a pair of glasses tinted a pale yellow, with shades at
the sides; and in spite of this protection she was so annoyed by the
light that her eyes were almost closed, and she had great difficulty
in finding her way about the room. Her vision without glasses was
3/200. All reading had been forbidden, playing the piano from the
notes was not allowed, and she had been obliged to give up the idea
of going to college. The sensitiveness to light was relieved in a few
minutes by focussing the light of the sun upon the upper part of the
eyeball when she looked far down, by means of a burning glass (see
Chapter XVII). The patient was then seated before a Snellen test card
and directed to look away from it, rest her eyes, and then look at
the big C. For a fraction of a second her vision was improved, and by
frequent
demonstrations she was made to realize that any effort to see the
letters always lowered the vision. By alternately looking away, and
then looking back at the letters for a fraction of a second, her
vision improved so rapidly that in the course of half an hour it was
almost normal for the distance. Then diamond type was given her to
read.
The
attempt to read it at once brought on a severe pain. She was directed
to proceed as she had in reading the Snellen test card; and in a few
minutes, by alternately looking away and then looking at the first
letter of each word in turn, she became able to read without fatigue,
discomfort, or pain. She left the office without her glasses, and was
able to see her way without difficulty. Other patients have been
benefited as promptly by this simple method.
CITATIONS
1.
Double and multiple vision.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XVI
THE ILLUSIONS OF IMPERFECT AND OF NORMAL SIGHT
Persons
with imperfect sight always have illusions of vision; so do persons
with normal sight. But while the illusions of normal sight are an
evidence of relaxation, the illusions of imperfect sight are an
evidence of strain. Some persons with errors of refraction have few
illusions, others have many; because the strain which causes the
error of refraction is not the same strain that is responsible for
the illusions.
The
illusions of imperfect sight may relate to the color, size, location
and form of the objects regarded. They may include appearances
of things that have no existence at all, and various other curious
and interesting manifestations.
ILLUSIONS
OF COLOR
When
a patient regards a black letter and believes it to be grey, yellow,
brown, blue, or green, he is suffering from an illusion of color.
This phenomenon differs from colorblindness. The color-blind person
is unable to differentiate between different colors, usually blue and
green, and his inability to do so is constant. The person suffering
from an illusion of color does not see the false colors constantly or
uniformly. When he looks at the Snellen test card the black letters
may appear to him at one time to be grey; but at another moment they
may appear to be a shade of yellow, blue, or brown. Some patients
always see the black letters red; to others they appear red only
occasionally. Although the letters are all of the same color, some
may see the large letters black and the small ones yellow or blue.
Usually the large letters are seen darker than the small ones,
whatever color they appear to be. Often
different
colors appear in the same letter, part of it seeming to be black,
perhaps, and the rest grey or some other color. Spots of black, or of
color, may appear on the white; and spots of white, or of color, on
the black.
ILLUSIONS
OF SIZE
Large
letters may appear small, or small letters large. One letter may
appear to be of normal size, while another of the same size and at
the same distance may appear larger or smaller than normal. Or a
letter may appear to be of normal size at the near-point and at the
distance, and only half that size at the middle distance. When a
person can judge the size of a letter correctly at all distances up
to twenty feet his vision is normal. If the size appears different to
him at different distances, he is suffering from an illusion of size.
At great distances the judgment of size is always imperfect,
because the sight at such distances is imperfect, even though perfect
at ordinary distances. The stars appear to be dots, because the eye
does not possess perfect vision for objects at such distances. A
candle seen half a mile away appears smaller than at the near-point;
but seen through a telescope giving perfect vision at that distance
it will be the same as at the near-point. With improved vision the
ability to judge size improves.
The
correction of an error of refraction by glasses seldom enables the
patient to judge size as correctly as the normal eye does, and
the ability to do this may differ very greatly in persons having the
same error of refraction. A person with ten diopters of myopia
corrected by glasses may (rarely) be able to judge the sizes of
objects correctly. Another person, with the same degree of myopia and
the same glasses, may see them only one-half or one-third their
normal size. This indicates that errors of refraction have very
little to do with incorrect perceptions of size.
ILLUSIONS
OF FORM
Round
letters may appear square or triangular; straight letters may appear
curved; letters of regular form may appear very irregular; a round
letter may appear to have a checkerboard or a cross in the center. In
short, an infinite variety of changing forms may be seen.
Illumination, distance and environment are all factors in this form
of imperfect sight. Many persons can see the form of a letter
correctly when other letters are covered, but when the other letters
are visible they cannot see it. The indication of the position of a
letter by a pointer helps some people to see it. Others are so
disturbed by the pointer that they cannot see the letter so well.
ILLUSIONS
OF NUMBER
Multiple
images are frequently seen by persons with imperfect sight, either
with both eyes together, with each eye separately, or with only one
eye. The manner in which these multiple images make their appearance
is sometimes very curious. For instance, a patient with presbyopia
read the word HAS normally with both eyes. The word PHONES he
read correctly with the left eye; but when he read it with the right
eye he saw the letter P double, the imaginary image being a
little distance to the left of the real one. The left eye, while it
had normal vision for the word PHONES, multiplied the-shaft of a pin
when this object was in a vertical position (the head remaining
single), and multiplied the head when the position was changed to the
horizontal (the shaft then remaining single). When the point of the
pin was placed below a very small letter, the point was sometimes
doubled while the letter remained single. No error of refraction can
account for these phenomena. They are tricks of the mind only.
The ways in which multiple images are arranged are endless.
They
are sometimes placed vertically, sometimes horizontally or obliquely,
and sometimes in circles, triangles and other geometrical forms.
Their number, too, may vary from two to three, four, or more.
They may be stationary, or may change their position more or
less rapidly. They also show an infinite variety of color, including
a white even whiter than that of the background.
ILLUSIONS
OF LOCATION
A
period following a letter on the same horizontal level as the bottom
of the letter may appear to change its position in a great variety of
curious ways. Its distance from the letter may vary. It may even
appear on the other side of the letter. It may also appear above or
below the line. Some persons see letters arranged in irregular order.
In the case of the word AND, for instance, the D may occupy the place
of the N. or the first letter may change places with the last. All
these things are mental illusions. The letters sometimes appear to be
farther off than they really are. The small letters, twenty feet
distant, may appear to be a mile away. Patients troubled by illusions
of distance sometimes ask if the position of the card has not been
changed.
ILLUSIONS
OF NON-EXISTENT OBJECTS
When
the eye has imperfect sight the mind not only distorts what the eye
sees, but it imagines that it sees things that do not exist. Among
illusions of this sort are the floating specks which so often appear
before the eyes when the sight is imperfect, and even when it is
ordinarily very good. These specks are known scientifically as
"muscae volitantes," or "flying flies," and
although they are of no real importance, being symptoms of
nothing except mental strain, they have attracted so much
attention, and usually cause so much alarm to the patient, that they
will be discussed at length in another chapter.
ILLUSIONS
OF COMPLEMENTARY COLORS
When
the sight is imperfect the subject, on looking away from a black,
white, or brightly colored object, and closing the eyes, often
imagines for a few seconds that he sees the object in a
complementary, or approximately complementary, color. If the object
is black upon a white background, a white object upon a black
background will be seen. If the object is red, it may be seen as
blue; and if it is blue, it may ap
pear
to be red. These illusions, which are known as "after-images,"
may also be seen, though less commonly, with the eyes open, upon
any background at which the subject happens to look, and are often so
vivid that they appear to be real.
ILLUSIONS
OP THE COLOR OF THE SUN
Persons
with normal sight see the sun white, the whitest white there is; but
when the sight is imperfect it may appear to be any color in the
spectrum - red, blue, green, purple, yellow, etc. In fact, it has
even been described by persons with imperfect vision as totally
black. The setting sun commonly appears to be red, because of
atmospheric conditions; but in many cases these conditions are
not such as to change the color, and while this still appears to be
red to persons with imperfect vision, to persons with normal vision
it appears to be white. When the redness of a red sun is an illusion,
and not due to atmospheric conditions, its image on the ground glass
of a camera will be white, not red, and the rays focussed with a
burning glass will also be white. The same is true of a red moon.
BLIND
SPOTS AFTER LOOKING AT THE SUN
After
looking at the sun most people see black or colored spots which may
last from a few minutes to a year or longer, but are never permanent.
These spots are also illusions, and are not due, as is commonly
supposed, to any organic change in the eye. Even the total blindness
which sometimes results, temporarily, from looking at the sun, is
only an illusion.
ILLUSIONS
OF TWINKLING STARS
The
idea that the stars should twinkle has been embodied in song and
story, and is generally accepted as part of the natural order of
things; but it can be demonstrated that this appearance is simply an
illusion of the mind.
CAUSE
OF THE ILLUSIONS OF IMPERFECT SIGHT
All
the illusions of imperfect sight are the result of a strain of the
mind, and when the mind is disturbed for any reason illusions of all
kinds are very likely to occur. This strain is not only different
from the strain that produces the error of refraction, but it can be
demonstrated that for each and every one of these illusions there is
a different kind of strain. Alterations of color do not necessarily
affect the size or form of objects, or produce any other illusion,
and it is possible to see the color of a letter, or of a part of a
letter, perfectly, without recognizing the letter. To change black
letters into blue, or yellow, or another color, requires a
subconscious strain to remember or imagine the colors concerned,
while to alter the form requires a subconscious strain to see the
form in question. With a little practice anyone can learn to
produce illusions of form and color by straining consciously in the
same way that one strains unconsciously; and whenever illusions are
produced in this way it will be found that eccentric fixation
and an error of refraction have also been produced.
The
strain which produces polyopia is different again from the strain
which produces illusions of color, size and form. After a few
attempts most patients easily learn to produce polyopia at will.
Staring
or squinting, if the strain is great enough, will usually make one
see double. By looking above a light, or a letter, and then trying to
see it as well as when directly regarded, one can produce an illusion
of several lights, or letters, arranged vertically. If the strain is
great enough, there may be as many as a dozen of them. By looking to
the side of the light or letter, or looking away obliquely at any
angle, the images can be made to arrange themselves horizontally,
or obliquely at any angle.
To
see objects in the wrong location, as when the first letter of a word
occupies the place of the last, requires an ingenuity of eccentric
fixation and an education of the imagination which is unusual.
The
black or colored spots seen after looking at the sun, and the strange
colors which the sun sometimes seems to assume, are also the result
of the mental strain. When one becomes able to look at the orb of day
without strain, these phenomena immediately disappear.
After-images
have been attributed to fatigue of the retina, which is supposed to
have been so overstimulated by a certain color that it can no
longer perceive it, and therefore seeks relief in the hue which
is complementary to this color. If it gets tired looking at the
black C on the Snellen test card, for instance, it is supposed to
seek relief by seeing the C white. This explanation of the phenomenon
is very ingenious but scarcely plausible. The eyes cannot see when
they are closed;; and if they appear to see under these conditions,
it is obvious that the subject is suffering from a mental
illusion with which the retina has nothing to da. Neither can they
see what does not exist; and if they appear to see a white C on a
green wall where there is no such object, it is obvious again that
the subject is suffering from a mental illusion. The after-image
indicates, in fact, simply a loss of mental control, and occurs
when there is an error of refraction, because this condition also is
due to a loss of mental control. Anyone can produce an afterimage at
will by trying to see the big C all alike - that is, under a strain;
but one can look at it indefinitely by central fixation without any
such result.
While
persons with imperfect sight usually see the stars twinkle, they do
not necessarily do so. Therefore it is evident that the strain
which causes the twinkling is different from that which causes the
error of refraction. If one can look at a star without trying to see
it, it does not twinkle; and when the illusion of twinkling has been
produced, one can usually stop it by "swinging" the
star. On the other hand, one can start the planets, or even the moon,
to twinkling, if one strains sufficiently to see them.
ILLUSIONS
OF NORMAL SIGHT
The
illusions of normal sight include all the phenomena of central
fixation. When the eye with normal sight looks at a letter on the
Snellen test card, it sees the point fixed best,- and everything else
in the field of vision appears less distinct. As a matter of fact,
the whole letter and all the letters may be perfectly black and
distinct, and the impression that one letter is blacker than the
others, or that one part of a letter is blacker than the rest, is an
illusion. The normal eye, however, may shift so rapidly that it
appears to see a whole line of small letters all alike
simultaneously. As a matter of fact there is, of course, no such
picture on the retina. Each letter has not only been seen separately,
but it has been demonstrated in the chapter on "Shifting and
Swinging" that if the letters are seen at a distance of fifteen
or twenty feet, they could not be recognized unless about four
shifts were made on each letter. To produce the impression of a
simultaneous picture of fourteen letters, therefore, some sixty or
seventy pictures, each with some one point more distinct than the
rest, must have been produced upon the retina. The idea that the
letters are seen all alike simultaneously is, therefore, an illusion.
Here we have two different kinds of illusions. In the first case the
impression made upon the brain is in accordance with the picture on
the retina, but not in accordance with the fact. In the second the
mental impression is in accordance with the fact, but not with the
pictures upon the retina.
The
normal eye usually sees the background of a letter whiter than it
really is. In looking at the letters on the Snellen test card it sees
white streaks at the margins of the letters, and in reading fine
print it sees between the lines and the letters, and in the openings
of the letters, a white more intense than the reality. Persons who
cannot read fine print may see this illusion, but less clearly. The
more clearly it is seen, the better the vision; and if it can be
imagined consciously - it is imagined
unconsciously
when the sight is normal - the vision improves. If the lines of
fine type are covered, the streaks between them disappear. When the
letters are regarded through a magnifying glass by the eye with
normal sight, the illusion is not destroyed, but the intensity of the
white and black are lessened. With imperfect sight it may be
increased to some extent by this means, but will remain less intense
than the white and black seen by the normal eye. The facts
demonstrate that perfect sight cannot be obtained with glasses.
The
illusions of movement produced by the shifting of the eye and
described in detail in the chapter on "Shifting and Swinging"
must also be numbered among the illusions of normal sight, and so
must the perception of objects in an upright position. This last is
the most curious illusion of all. No matter what the position of the
head, and regardless of the fact that the image on the retina is
inverted, we always see things right side up.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XVII
VISION UNDER ADVERSE CONDITIONS A BENEFIT TO THE EYES
According
to accepted ideas of ocular hygiene, it is important to protect the
eyes from a great variety of influences which are often very
difficult to avoid, and to which most people resign themselves with
the uneasy sense that they are thereby "ruining their eyesight."
Bright lights, artificial lights, dim lights, sudden fluctuations of
light, fine print, reading in moving vehicles, reading lying down,
etc., have long been considered "bad for the eyes," and
libraries of literature have been produced about their
supposedly direful effects. These ideas are diametrically
opposed to the truth. When the eyes are properly used, vision under
adverse conditions not only does not injure them, but is an actual
benefit, because a greater degree of relaxation is required to see
under such conditions than under more favorable ones. It is true that
the conditions in question may at first cause discomfort, even to
persons with normal vision; but a careful study of the facts has
demonstrated that only persons with imperfect sight suffer seriously
from them, and that such persons, if they practice central fixation,
quickly become accustomed to them and derive great benefit from them.
Although
the eyes were made to react to the light, a very general fear of the
effect of this element upon the organs of vision is entertained both
by the medical profession and by the laity. Extraordinary
precautions are taken in our homes, offices and schools to
temper the light, whether natural or artificial, and to insure that
it shall not shine directly into the eyes; smoked and amber glasses,
eye-shades, broad-brimmed hats and parasols are commonly used to
protect the organs of vision from what is considered an excess of
light; and when actual disease is
present,
it is no uncommon thing for patients to be kept for weeks, months and
years in dark rooms, or with bandages over their eyes.
The
evidence on which this universal fear of the light has been based is
of the slightest. In the voluminous literature of the subject
one finds such a lack of information that in 1910 Dr J. Herbert
Parsons of the Royal Ophthalmic Hospital of London, addressing a
meeting of the Ophthalmological Section of the American Medical
Association, felt justified in saying that ophthalmologists, if
they were honest with themselves, "must confess to a lamentable
ignorance of the conditions which render bright light deleterious to
the eyes."(1) Since then, Verhoeff and Bell have reported(2) an
exhaustive series of experiments carried on at the Pathological
Laboratory of the Massachusetts Charitable Eye and Ear Infirmary,
which indicate that the danger of injury to the eye from light
radiation as such has been "very greatly exaggerated." That
brilliant sources of light sometimes produce unpleasant temporary
symptoms cannot, of course, be denied; but as regards definite
pathological effects, or permanent impairment of vision from
exposure to light alone, Drs. Verhoeff and Bell were unable to find,
either clinically or experimentally, anything of a positive nature.
As
for danger from the heat effects of light, they consider this to be
"ruled out of consideration by the immediate discomfort produced
by excessive heat." They conclude, in short, that "the eye
in the process of evolution has acquired the ability to take care of
itself under extreme conditions of illumination to a degree
hitherto deemed highly improbable." In their experiments,
the eyes of rabbits, monkeys and human beings were flooded for an
hour or more with light of extreme intensity, without any sign of
permanent injury, the resulting scotomata(3) disappearing within a
few hours. Commercial illuminants were found to be entirely free
of danger under any ordinary conditions of their use. It was even
found impossible to damage the retina with any artificial
illuminant, except by exposures and intensities
enormously
greater than any likely to occur outside the laboratory. In one case
an animal succumbed to heat after an exposure of an hour and a half
to a 750-watt nitrogen lamp at twenty centimeters-about eight inches;
but in a second experiment, in which it was well protected from the
heat, there was no damage to the eye whatever after an exposure
of two hours. As for the ultra violet part of the spectrum, to which
exaggerated importance has been attached by many recent writers, the
situation was found to be much the same as with respect to the rest
of the spectrum; that is, "while under conceivable or
realizable conditions of overexposure injury may be done to the
external eye, yet under all practicable conditions found in actual
use of artificial sources of light for illumination the ultra violet
part of the spectrum may be left out as a possible source of injury."
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XVII
VISION UNDER ADVERSE CONDITIONS A BENEFIT TO THE EYES
According
to accepted ideas of ocular hygiene, it is important to protect the
eyes from a great variety of influences which are often very
difficult to avoid, and to which most people resign themselves with
the uneasy sense that they are thereby "ruining their eyesight."
Bright lights, artificial lights, dim lights, sudden fluctuations of
light, fine print, reading in moving vehicles, reading lying down,
etc., have long been considered "bad for the eyes," and
libraries of literature have been produced about their supposedly
direful effects. These ideas are diametrically opposed to the truth.
When the eyes are properly used, vision under adverse conditions not
only does not injure them, but is an actual benefit, because a
greater degree of relaxation is required to see under such conditions
than under more favorable ones. It is true that the conditions in
question may at first cause discomfort, even to persons with normal
vision; but a careful study of the facts has demonstrated that only
persons with imperfect sight suffer seriously from them, and that
such persons, if they practice central fixation, quickly become
accustomed to them and derive great benefit from them.
Although
the eyes were made to react to the light, a very general fear of the
effect of this element upon the organs of vision is entertained both
by the medical profession and by the laity. Extraordinary
precautions are taken in our homes, offices and schools to temper the
light, whether natural or artificial, and to insure that it shall not
shine directly into the eyes; smoked and amber glasses,
eye-shades, broad-brimmed hats and parasols are commonly used to
protect the organs of vision from what is considered an excess of
light; and when
actual
disease is present, it is no uncommon thing for patients to be kept
for weeks, months and years in dark rooms, or with bandages over
their eyes.
The
evidence on which this universal fear of the light has been based is
of the slightest. In the voluminous literature of the subject one
finds such a lack of information that in 1910 Dr J. Herbert Parsons
of the Royal Ophthalmic Hospital of London, addressing a meeting of
the Ophthalmological Section of the American Medical
Association, felt justified in saying that ophthalmologists, if
they were honest with themselves, "must confess to a lamentable
ignorance of the conditions which render bright light deleterious to
the eyes."(1) Since then, Verhoeff and Bell have reported(2) an
exhaustive series of experiments carried on at the Pathological
Laboratory of the Massachusetts Charitable Eye and Ear Infirmary,
which indicate that the danger of injury to the eye from light
radiation as such has been "very greatly exaggerated." That
brilliant sources of light sometimes produce unpleasant temporary
symptoms cannot, of course, be denied; but as regards definite
pathological effects, or permanent impairment of vision from exposure
to light alone, Drs. Verhoeff and Bell were unable to find, either
clinically or experimentally, anything of a positive nature.
As
for danger from the heat effects of light, they consider this to be
"ruled out of consideration by the immediate discomfort produced
by excessive heat." They conclude, in short, that "the eye
in the process of evolution has acquired the ability to take care of
itself under extreme conditions of illumination to a degree
hitherto deemed highly improbable." In their experiments,
the eyes of rabbits, monkeys and human beings were flooded for an
hour or more with light of extreme intensity, without any sign of
permanent injury, the resulting scotomata(3) disappearing within a
few hours. Commercial illuminants were found to be entirely free
of danger under any ordinary conditions of their use. It was
even found impossible to damage the retina with any artificial
illuminant, except by exposures and intensities enormously greater
than any likely to occur outside the laboratory. In one case an
animal succumbed to heat after an exposure of an hour and a half to a
750-watt nitrogen lamp at twenty centimeters-about eight inches; but
in a second experiment, in which it was well protected from the heat,
there was no damage to the eye whatever after an exposure of two
hours. As for the ultra violet part of the spectrum, to which
exaggerated importance has been attached by many recent writers, the
situation was found to be much the same as with respect to the rest
of the spectrum; that is, "while under conceivable or
realizable conditions of overexposure injury may be done to the
external eye, yet under all practicable conditions found in actual
use of artificial sources of light for illumination the ultra violet
part of the spectrum may be left out as a possible source of injury."

Fig.
46. Woman With Normal Vision Looking Directly at the Sun. Note That
the Eyes are Wide Open and That There Is No Sign of Discomfort.
The
results of these experiments are in complete accord with my own
observations as to the effect of strong light upon the eyes. In my
experience such light has never been permanently injurious. Persons
with normal sight have been able to look at the sun for an indefinite
length of time, even an hour or longer, without any discomfort or
loss of vision. Immediately afterward they were able to read the
Snellen test card with improved vision, their sight having become
better than what is ordinarily considered normal. Some persons with
normal sight do suffer discomfort and loss of vision when they look
at the sun; but in such cases the retinoscope always indicates an
error of refraction, showing that this condition is due, not to the
light, but to strain. In exceptional cases persons with defective
sight have been able to look at the sun, or have thought that they
have looked at it, without discomfort and without loss of vision;
but, as a rule, the strain in such eyes is enormously increased and
the vision decidedly lowered by sungazing, as manifested by inability
to read the Snellen test card. Blind areas (scotomata) may develop in
various parts of the field-two or three or more. The sun, instead of
appearing perfectly white, may appear to be slate-colored, yellow,
red, blue, or even totally black. After looking away from the sun,
patches of color of various kinds and sizes may be seen, continuing a
variable length of time, from a few seconds to a few minutes, hours,
or even months. In fact, one patient was troubled in this way for a
year or more after looking at the sun for a few seconds. Even total
blindness lasting a few hours has been produced. Organic changes may
also be produced. Inflammation, redness of the conjunctiva,
cloudiness of the lens and of the aqueous and vitreous humors,
congestion and cloudiness of the retina, optic nerve and choroid,
have all resulted from sun-gazing. These effects, however, are always
temporary. The scotomata, the strange colors, even the total
blindness, as explained in the preceding chapter, are only
mental illusions. No matter how much the sight may have been impaired
by sun-gazing, or how long the impairment may have lasted. a return
to normal has always occurred; while prompt relief of all the
symptoms mentioned has always followed the relief of eyestrain,
showing that the conditions are the result, not of the light, but of
the strain. Some persons who have believed their eyes to have been
permanently injured by the sun have been promptly cured by central
fixation, indicating that their blindness had been simply functional.
By
persistence in looking at the sun, a person with normal sight soon
becomes able to do so without any loss of vision; but persons with
imperfect sight usually find it impossible to accustom themselves to
such a strong light until their vision has been improved by other
means. On has to be very careful in recommending sun-gazing to
persons with imperfect sight; because although no permanent harm can
result from it, great temporary discomfort
may
be produced,
with no permanent benefit. In some rare cases, however, complete
cures have been effected by this means alone.
In
one of these cases the sensitiveness of the patient, even to ordinary
daylight, was 60 great that an eminent specialist had felt justified
in putting a black bandage over one eye and covering the other with a
smoked glass so dark as to be nearly opaque. She was kept in this
condition of almost total blindness for two years without any
improvement. Other treatment extending over some months also failed
to produce satisfactory results. She was then advised to look
directly at the sun. The immediate result was total blindness, which
lasted several hours; but next day the vision was not only restored
to its former condition, but was improved. The sungazing was
repeated, and each time the blindness lasted for a shorter period. At
the end of a week the patient was able to look directly at the sun
without discomfort, and her vision, which had been 20/200 without
glasses and 20/70 with them, had improved to 20/10, twice the
accepted standard for normal vision.
Patients
of this class have also been greatly benefited by focussing the rays
of the sun directly upon their eyes, marked relief being often
obtained in a few minutes.

Like
the sun, a strong electric light may also lower
the
vision temporarily, but never does any permanent harm. In those
exceptional cases in which the patient can become accustomed to the
light, it is beneficial. After looking at a strong electric light
some patients have been able to read the Snellen test card better.
It
is not light but darkness that is dangerous to the eye. Prolonged
exclusion from the light always lowers the vision, and may produce
serious inflammatory conditions. Among young children living in
tenements this is a somewhat frequent cause of ulcers upon the
cornea, which ultimately destroy the sight. The children, finding
their eyes sensitive to light, bury them in the pillows and thus shut
out the light entirely. The universal fear of reading or doing fine
work in a dim light is, however, unfounded. So long as the light is
sufficient so that one can see without discomfort, this practice is
not only harmless, but may be beneficial.
Sudden
contrasts of light are supposed to be particularly harmful to the
eye. The theory on which this idea is based is summed up as follows
by Fletcher B. Dresslar, specialist in school hygiene and sanitation
of the United States Bureau of Education:
"The
muscles of the iris are automatic in their movements, but rather
slow. Sudden contrasts of strong light and weak illumination are
painful and likewise harmful to the retina. For example, if the eye,
adjusted to a dim light, is suddenly turned toward a brilliantly
lighted object, the retina will receive too much light and will be
shocked before the muscles controlling the iris can react to shut out
the superabundance of light. If contrasts are not strong, but
frequently made, that is, if the eye is called upon to function where
frequent adjustments in this way are necessary, the muscles
controlling the iris become fatigued, respond more slowly and less
perfectly. As a result, eyestrain in the ciliary muscles is produced
and the retina is over-stimulated. This is one cause of headaches and
tired eyes."(4)
There
is no evidence whatever to support these statements. Sudden
fluctuations of light undoubtedly cause discomfort to many
persons, but, far from being injurious, I have found them, in all
cases observed, to be actually beneficial. The
Fig.
48. Focussing the Rays of the Sun Upon the Eye of a Patient by Means
of a Burning Glass. --
pupil
of the normal eye, when it has normal sight, does not change
appreciably under the influence of changes of illumination; and
persons with normal vision are not inconvenienced by such changes. I
have seen a patient look directly at the sun after coming from an
imperfectly lighted room, and then, returning to the room,
immediately pick up a newspaper and read it. When the eye has
imperfect sight, the pupil usually contracts in the light and expands
in the dark, but it has been observed to contract to the size of a
pinhole in the dark. Whether the contraction takes place under the
influence of light or of darkness, the cause is the same, namely,
strain. Persons with imperfect sight suffer great inconvenience,
resulting in lowered vision, from changes in the intensity of the
light; but the lowered vision is always temporary, and if the eye is
persistently exposed to these conditions, the sight is benefited.
Such practices as reading alternately in a bright and a dim light, or
going from a dark room to a well-lighted one, and vice versa, are to
be recommended. Even such rapid and violent fluctuations of light as
those involved in the production of the moving picture are, in the
long run, beneficial to all eyes. I always advise patients under
treatment for the cure of defective vision to go to the movies
frequently and practice central fixation. They soon become accustomed
to the flickering light, and afterward other light and reflections
cause less annoyance.
Reading
is supposed to be one of the necessary evils of civilization; but it
is believed that by avoiding fine print, and taking care to read only
under certain favorable conditions, its deleterious influences can be
minimized. Extensive investigations as to the effect of various
styles of print on the eyesight of school children have been made,
and detailed rules have been laid down as to the size of the print,
its shading, the distance of the letters from each other, the spaces
between the lines, the length of the lines, etc.. As regards the
effects of different sorts of type on the human eye in general and
those of children in particular, Dr. A. G. Young, in his much quoted
report(5) to the Maine State Board of Health makes the following
interesting observations:
“Pearl,”
as the printers call it, is unfit for any eves, yet the piles of
Bibles and Testaments annually printed in it tempt many eyes to
self-destruction.
“Agate“
is the type in which a boy, to the writer's knowledge, undertook to
read the Bible through, His outraged eyes broke down with asthenopia
before he went far and could be used but little for school work the
next two years.
“Nonpareil”
is used in some papers and magazines for children, but, to spare the
eyes, all such should, and do, go on the list of forbidden reading
matter in those homes where the danger of such print is understood.
“Minion”
is read by the healthy, normal young eye without appreciable
difficulty, but even to the sound eye the danger of strain is so
great that all books and magazines for children printed from it
should be banished from the home and school.
“Brevier”
is much used in newspapers, but is too small for magazines or books
for young folks.
“Bourgeois”
is much used in magazines, but should he used in only those school
books to which a brief reference is made.
“Long
Primer” is suitable for school readers for the higher and
intermediate grades, and for text books generally.
“Small
Pica” is still a more luxurious type, used in the North
American Review and the Forum.
“Pica”
is a good type for books for small children.
“Great
Primer” should be used for the first reading book.
All
this is directly contrary to my own experience. Children might be
bored by books in excessively small print; but I have never seen any
reason for supposing that their eyes, or any other eyes, would be
harmed by such type. On the contrary, the reading of fine print,
when it can be done without discomfort, has invariably
proven to be beneficial, and the dimmer the light in which it can be
read, and the closer to the eyes it can be held, the greater the
benefit. By this means severe pain in the eyes has been relieved in a
few minutes or even instantly. The reason is that fine print cannot
be read in a dim light and close to the eyes unless the eyes are
relaxed, whereas large print can be read in a good light and at
ordinary reading distance although the eyes may be under a strain.
When fine print can be read under adverse conditions, the reading of
ordinary print under ordinary conditions is vastly improved. In
myopia it may be a benefit to strain to see fine print, because
myopia is always lessened when there is a strain to see near objects,
and this has sometimes counteracted the tendency to strain in looking
at distant objects, which is always associated with the production of
myopia. Even straining to see print so fine that it cannot be
read is a benefit to some myopes.
Persons
who wish to preserve their eyesight are frequently warned not to read
in moving vehicles; but since under modern conditions of life many
persons have to spend a large part of their time in moving vehicles,
and many of them have no other time to read, it is useless to expect
that they will ever discontinue the practice. Fortunately the theory
of its injuriousness is not borne out by the facts. When the object
regarded is moved more or less rapidly, strain and lowered vision
are, at first, always produced; but this is always temporary, and
ultimately the vision is improved by the practice.
There
is probably no visual habit against which we have been more
persistently warned than that of reading in a recumbent posture. Many
plausible reasons have been adduced for its supposed injuriousness;
but so delightful is the practice that few, probably, have ever been
deterred from it by fear of the consequences. It is gratifying to be
able to state, therefore, that I have found these consequences to be
beneficial rather than injurious. As in the case of the use of the
eyes under other difficult conditions, it is a good thing to be able
to read lying down, and the ability to do it improves with practice.
In an upright position, with a good light coming over the left
shoulder, one can read with the eyes under a considerable degree of
strain; but in a recumbent posture, with the light and the angle of
the page to the eye unfavorable, one cannot read unless one relaxes.
Anyone who can read lying down without discomfort is not likely to
have any difficulty in reading under ordinary conditions.
The
fact is that vision under difficult conditions is good mental
training. The mind may be disturbed at first by the unfavorable
environment; but after it has become accustomed to such environments,
the mental control, and, consequently, the eyesight are improved. To
advise against using the eyes under unfavorable conditions is like
telling a person who has been in bed for a few weeks and finds it
difficult to walk to refrain from such exercise. Of course,
discretion must be used in both cases. The convalescent must not at
once try to run a Marathon, nor must the person with defective
vision attempt, without some preparation, to outstare the sun at
noonday. But just as the invalid may gradually increase his strength
until the Marathon has no terrors for him, so may the eye with
defective sight be educated until all the rules with which we have so
long allowed ourselves to be harassed in the name of "eye
hygiene" may be disregarded, not only with safety but with
benefit.
Fig.
49. Specimen of Diamond Type -- Many patients have been
greatly benefited by reading type of this size. [Note: Although the
sample from Bates's book is diamond type, the sample above is a
retype for the sake of readability and will vary on different
computers. - DK]

Fig.
50. Photographic Type Reduction -- Patients who can read
photographic type reductions are instantly relieved of pain and
discomfort when they do so and those who cannot read such type may be
benefited simply by looking at it. [Note: Although the sample from
Bates's book is clear enough to be readable, the converted picture
above is of too low quality to be readable. - DK]
CITATIONS
1.
Jour. Am. Med. Assn., Dec. 10, 1910, p. 2028.
2.
Proc. Am. Acad. Arts and Sciences, 1916, Vol. 51, No. 13.
3.
Blind areas.
4.
School Hygiene, Brief Course Series in Education, edited by Monroe,
1916, p. 240.
5.
Seventh Annual Report to the Maine State Board of Health, by the
secretary, Dr. A. G. Young, 1891, p. 193.
|
Seven
Truths of Normal Sight
|
|
1--Normal
Sight can always be demonstrated in the normal eye, but only under
favorable conditions.
|
|
2--Central
Fixation: The letter or part of the letter regarded is always seen
best.
|
|
3--Shifting:
The point regarded changes rapidly and continuously.
|
|
4--Swinging:
When the shifting is slow, the letters appear to move from side to
side or in other directions with a pendulum-like motion.
|
|
5--Memory
is perfect The color and background of the letters, or other
objects seen are remembered perfectly, instantaneously and
continuously.
|
|
6--Imagination
is good. One may even see the white part of the letters whiter
than it really is, while the black is not altered by distance,
illumination, size, or form, of the letters.
|
|
7--Rest
or relaxation of the eye and mind is perfect and can always be
demonstrated.
|
|
When
one of these seven fundamentals is perfect all are perfect.
|
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XVIII
OPTIMUMS AND PESSIMUMS
In
nearly all cases of imperfect sight due to errors of refraction there
is some object, or objects, which can be regarded with normal vision.
Such objects I have called "optimums." On the other hand,
there are some objects which persons with normal eyes and ordinarily
normal sight always see imperfectly, an error of refraction being
produced when they are regarded, as demonstrated by the retinoscope.
Such objects I have called "pessimums." An object
becomes an optimum, or a pessimum, according to the effect it
produces upon the mind, and in some cases this effect is easily
accounted for.
For
many children their mother's face is an optimum, and the face of
a stranger a pessimum. A dressmaker was always able to thread a No.
10 needle with a fine thread of silk without glasses, although she
had to put on glasses to sew on buttons, because she could not
see the holes. She was a teacher of dressmaking, and thought the
children stupid because they could not tell the difference between
two different shades of black. She could match colors without
comparing the samples. Yet she could not see a black line in a
photographic copy of the Bible which was-no finer than a thread of
silk, and she could not remember a black period. An employee in a
cooperage factory, who had been engaged for years in picking out
defective barrels as they went rapidly past him on an inclined plane,
was able to continue his work after his sight for most other objects
had become very defective, while persons with much better sight for
the Snellen test card were unable to detect the defective barrels.
The familiarity of these various objects made it possible for the
subjects to look at them without strain - that is, without trying to
see them. Therefore the barrels were to the cooper optimums;
while
the needle's eye and the colors of silk and fabrics were optimums to
the dressmaker. Unfamiliar objects, on the contrary, are always
pessimums, as pointed out in the chapter on "The Variability of
the Refraction of the Eye."
In
other cases there is no accounting for the idiosyncrasy of the
mind which makes one object a pessimum and another an
optimum. It is also impossible to account for the fact that an object
may be an optimum for one eye and not for the other, or an optimum at
one time and at one distance and not at others. Among these
unaccountable optimums one often finds a particular letter on the
Snellen test card. One patient, for instance, was able to see the
letter K on the forty, fifteen and ten lines, but could see none of
the other letters on these lines, although most patients would see
some of them, on account of the simplicity of their outlines, better
than they would such a letter as K.
Pessimums
may be as curious and unaccountable as optimums. The letter V is 50
simple in its outlines that many people can see it when they cannot
see others on the same line. Yet some people are unable to
distinguish it at any distance, although able to read other letters
in the same word, or on the same line of the Snellen test card. Some
people again will not only be unable to recognize the letter V in a
word, but also to read any word that contains it, the pessimum
lowering their sight not only for itself but for other objects. Some
letters, or objects, become pessimums only in particular situations.
A letter, for instance, may be a pessimum when located at the end or
at the beginning of a line or sentence, and not in other places. When
the attention of the patient is called to the fact that a letter seen
in one location ought logically to be seen equally well in others,
the letter often ceases to be a pessimum in any situation.
A
pessimum, like an optimum, may be lost and later become manifest. It
may vary according to the light and distance. An object which is a
pessimum in a moderate light may not be so when the light is
increased or diminished. A pessimum at twenty feet
may
not be one at two feet, or thirty feet, and an object which is a
pessimum when directly regarded may be seen with normal vision in the
eccentric field.
For
most people the Snellen test card is a pessimum. If you can see the
Snellen test card with normal vision, you can see almost anything
else in the world. Patients who cannot see the letters on the Snellen
test card can often see other objects of the same size and at the
same distance with normal sight. When letters which are seen
imperfectly, or even letters which cannot be seen at all, or which
the patient is not conscious of seeing are regarded, the error of
refraction is increased. The patient may regard a blank white card
without any error of refraction; but if he regards the lower part of
a Snellen test card, which appears to him to be just as blank as the
blank card, an error of refraction can always be demonstrated, and if
the visible letters of the card are covered, the result is the same.
The pessimum may, in short, be letters or objects which the patient
is not conscious of seeing. This phenomenon is very common. When
the card is seen in the eccentric field it may have the effect of
lowering the vision for the point directly regarded. For
instance, a patient may regard an area of green wallpaper at the
distance, and see the color as well as at the near-point; but if a
Snellen test card on which the letters are either seen imperfectly,
or not seen at all, is placed in the neighborhood of the area being
regarded, the retinoscope may indicate an error of refraction. When
the vision improves the number of letters on the card which are
pessimums diminishes and the number of optimums increases, until the
whole card becomes an optimum.
A
pessimum, like an optimum, is a manifestation of the mind. It is
something associated with a strain to see, just as an optimum is
something which has no such association. It is not caused by the
error of refraction, but always produces an error of refraction;
and when the strain has been relieved it ceases to be a pessimum and
becomes an optimum.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XIX
THE RELIEF OF PAIN AND OTHER SYMPTOMS BY THE AID OF THE
MEMORY
Many
years ago patients who had been cured of imperfect sight by treatment
without glasses quite often told me that after their vision had
become perfect they were always relieved of pain, not only in the
eyes and head, but in other parts of the body, even when the pain was
apparently caused by some organic disease, or by an injury. The
relief in many cases was so striking that I investigated some
thousands of cases and found it to be a fact that persons with
perfect sight, or the memory of perfect sight - that is, of
something perfectly seen - do not suffer pain in any part of the
body, while by a strain or effort to see I have produced pain in
various parts of the body.
By
perfect sight is not meant, necessarily, the perfect visual
perception of words, letters, or objects, of a more or less
complicated form. To see perfectly the color alone is sufficient, and
the easiest color to see perfectly is black. But perfect sight is
never continuous, careful scientific tests having shown that it is
seldom maintained for more than a few minutes and usually not so
long. For practical purposes in the relief of pain, therefore,
the memory is more satisfactory than sight.
When
black is remembered perfectly a temporary, if not a permanent, relief
of pain always results. The skin may be pricked with a sharp
instrument without causing discomfort. The lobe of the ear may be
pinched between the nails of the thumb and first finger, and no pain
will be felt. At the same time the sense of touch becomes more acute.
The senses of taste, smell and hearing are also improved, while the
efficiency of the mind is increased. The ability to
distinguish
different temperatures is increased, but one does not suffer from
heat or cold. Organic conditions may not be changed; but all of the
functional symptoms, such as fever, weakness, and shock, which
these conditions cause, are relieved. Patients who have learned to
remember black under all circumstances no longer dread to
visit the dentist.
When
they remember a period the drill causes them no pain, and they are
not annoyed even by the extraction of teeth. It is possible
to perform surgical operations without anaesthetics when the patient
is able to remember black perfectly. The following are only a few of
many equally striking cases which might be given of the relief or
prevention of pain by this means:

Fig.
51. Operating Without Anaesthetics --
The
patient suffered from ulceration of the eyeball resulting in the
formation of holes through which the fluids of the interior
escaped. These holes had to be closed by surgical operations,
and fourteen of these operations were performed without
anaesthetics, because the patient was able to prevent pain by
the memory of a black period.
A
patient suffered from ulceration of the eyeball, occurring at
different times and resulting in the formation of holes through which
the fluids in the interior escaped. These openings had to be closed
by surgical operations At first these operations were performed under
the influence of cocaine; but the progressive disease of the eye
caused so much congestion that complete anaesthesia was no longer
attainable
by the use of this drug, and ether and chloroform were employed. As
so many operations were needed, it became desirable to get along, if
possible, without anaesthetics, and the patient's success in
relieving pain by the memory of black suggested that she might also
be able to prevent the pain of operations in the same way. Her
ability to do this was tested by touching her eyeball lightly with a
blunt probe. At first she forgot the black as soon as the probe
touched her eye, but later she became able to remember it. The
operation was then successfully performed; the patient not only felt
no pain, but her self-control was better than when cocaine had been
used. Later fourteen more operations were performed under the
same conditions, the patient not only suffering no pain, but, what
was more remarkable, feeling no pain or soreness afterward. The
patient stated that if she had been operated upon by a stranger
she would probably have been so nervous that she would not have been
able to remember the black; but later she. was treated by a strange
dentist, who made two extractions and did some other work, all
without causing her any discomfort, because she was able to
remember the period perfectly.
A
man who had been extremely nervous in the dentist's chair, and
had had four- extractions made under gas, surprised his dentist,
after having learned the effect of the memory of a period
in-relieving pain, by having a tooth extracted without cocaine, gas,
or chloroform. The dentist complimented him on his nerve and
looked- incredulous when the patient said he had felt no pain at all.
In a second case, that of a woman, the dentist removed the nerve
from three teeth without causing the patient any pain.
A
boy of fourteen came to the eye clinic of the Harlem Hospital, New
York, with a foreign body deeply embedded in his cornea. It caused
him much pain, and his mother stated that a number of physicians
had been unable to remove it, because the child was so nervous that
he could not keep still long enough, although cocaine had been used
quite freely. The boy was told to look at a black object, close and
cover his eyes, and think of the black object until he saw black. He
was soon able to do this, and the pain in his eye was relieved. He
was next taught to remember the black with his eyes open. The
foreign body was then removed from the cornea. The operation was
one of much difficulty and required considerable time, but the
boy felt no pain. While it was in progress he was asked if he was
still remembering black.
"You
bet I am," he replied.
In
the same hospital a surgeon from the accident ward visited the eye
clinic with a friend suffering from pain in his eyes and head. The
patient was benefited very quickly by relaxation methods. The surgeon
said it was unusual, and spoke slightingly of my methods. I
challenged him to bring me a patient with pain that I could not
relieve in five minutes.
"All
right," he said. "I want you to understand that I am from
Missouri."
He
returned soon with a woman who had been suffering from severe
pains in her head for several years. She had been operated upon a
number of times, and had been under the care of the hospital for many
months.
"You
cannot help the pain in this patient's head," said the surgeon,
"because she has a brain tumor."
I
doubted the existence of a brain tumor, but I said: "Brain tumor
or no brain tumor, my assistant will stop the pain in five minutes."
He
took out his watch, opened it, looked at the time, and told my
assistant to go ahead. The patient was directed to look at a large
black letter, note its blackness, then to cover her closed eyes with
the palms of her hands, shutting out all the light, and to remember
the blackness of the letter until she saw everything black. In less
than three minutes she said:
"I
now see everything perfectly black. I feel no pain in my head. I am
completely relieved, and I thank you very much."
The
surgeon looked bewildered, and left the room without a word.

Fig.
52. Neuralgia Relieved by Palming and the Memory of Black --
While the visitor was explaining to her sceptical hostess the method
of relieving pain by palming and the memory of black another member
of the family, who was suffering from trigeminal neuralgia, came in,
and having heard what was being said, immediately put it into
practice and was cured. The hostess later developed severe pain in
her head and eyes, and did not obtain any relief until she also
practiced palming and the memory of black.
To
prevent a relapse the patient was advised to palm six times a day or
oftener. The pain did not return, and she came to the clinic some
weeks later to express her gratitude.
Not
only does the memory of perfect sight relieve pain and the symptoms
of disease, but in some cases it produces manifest relief of the
causes of these symptoms. Coughs, colds, hay fever, rheumatism and
glaucoma are among the conditions that have been relieved in this
way.
A
patient under treatment for imperfect sight from a high degree of
mixed astigmatism one day came to the office with a severe cold. She
coughed continually, and there was a profuse discharge from both
eyes and nose. There was some fever, with a severe pain in the eyes
and head, and the patient was unable to breathe through her nose
because of the inflammatory swelling. Palming was successful in
half an hour, when the pain and discharge ceased, the nose opened,
and the breathing and temperature became normal. The benefit was
permanent - a very unusual thing after one treatment.
A
boy of four with whooping-cough was always relieved by covering
his eyes and remembering black. The relapses became less frequent,
and in a few weeks he had completely recovered.
A
man who suffered every summer from attacks of hay fever, beginning in
June and lasting throughout the season, was completely relieved by
palming for half an hour; and after three years there had been no
relapse.
A
man of sixty-five who had been under treatment for rheumatism for six
months without improvement obtained temporary relief by palming, and
by the time his vision had become normal the relief of the rheumatism
was complete.
In
many cases of glaucoma not only the pain, but the tension which is
often associated with the pain, has been completely relieved by
palming. In some cases permanent relief of the tension has followed
one treatment. In others many treatments have been required.
Why
the memory of black should have this effect cannot be fully
explained, just as the action of many drugs cannot be explained; but
it is evident that the body must be less susceptible to disturbances
of all kinds when the mind is under control, and only when the mind
is under control can black be remembered perfectly. That pain can be
produced in any part of the body by the action of the mind is not a
new observation; and if the mind can produce pain, it is not
surprising that it should also be able to relieve pain and the
conditions which produce it. This, doubtless, is the explanation of
some of the remarkable cures reported by Faith Curists and
Christian Scientists. Whatever the explanation, however, the facts
have been attested by numerous proofs, and are of the greatest
practical value.
With
a little training anyone with good sight can be taught to remember
black perfectly with the eyes closed and covered, and with a little
more training anyone can learn to do it with the eyes open. When one
is suffering extreme pain, however, the control of the memory may be
difficult, and the assistance of someone who understands the method
may be necessary. With such assistance it is seldom or never
impossible.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XX
PRESBYOPIA: ITS CAUSE AND CURE
Among
people living under civilized conditions the accommodative power of
the eye gradually declines, in most cases, until at the age of sixty
or seventy it appears to have been entirely lost, the subject being
absolutely dependent upon his glasses for vision at the near-point.
As to whether the same thing happens among primitive people or
people living under primitive conditions, very little information is
available. Donders (1) says that the power of accommodation
diminishes little, if at all, more rapidly among people who use their
eyes much at the near-point than among agriculturists, sailors and
others who use them mainly for distant vision; and Roosa and
others(2) say the contrary. This is a fact however, that people who
cannot read, no matter what their age, will manifest a failure of
near vision if asked to look at printed characters, although their
sight for familiar objects at the near-point may be perfect. The fact
that such persons, at the age of forty-five or fifty, cannot
differentiate between printed characters is no warrant,
therefore, for the conclusion that their accommodative powers
are declining. A young illiterate would do no better, and a young
student who can read Roman characters at the near-point without
difficulty always develops symptoms of imperfect sight when he
attempts to read, for the first time, old English, Greek, or Chinese
characters.
When
the accommodative power has declined to the point at which reading
and writing become difficult the patient is said to have
"presbyopia," or, more popularly, "old sight";
and the condition is generally accepted, both by the popular and the
scientific mind, as one of the unavoidable inconveniences of old
age.
"Presbyopia," says Donders, "is the normal quality of
the normal, emmetropic eye in advanced age(3)," and similar
statements might be multiplied endlessly. De Schweinitz calls the
condition "a normal result of growing old";(4) according to
Fuchs it is "a physiological process which every eye
undergoes";(5) while Roosa speaks of the change as one
which "ultimately affects every eye."(6)
The
decline of accommodative power with advancing years is commonly
attributed to the hardening of the lens, an influence which is
believed to be augmented, in later years, by a flattening of
this body and a lowering of its refractive index, together with
weakness or atrophy of the ciliary muscle; and so regular is the
decline, in most cases, that tables have been compiled showing the
near-point to be expected at various ages. From these it is said one
might almost fit glasses without testing the vision of the subject;
or, conversely, one might, from a man's glasses, judge his age within
a year or two.
The
following table is quoted from Jackson's chapter on "The
Dioptrics of the Eye," in Norris and Oliver's "System of
Diseases of the Eye," (7) and does not differ materially from
the tables given by Fuchs, Donders and Duane. The first column
indicates the age, the second diopters of accommodative
power, the third the near-point for an emmetropic (8) eye, in
inches.
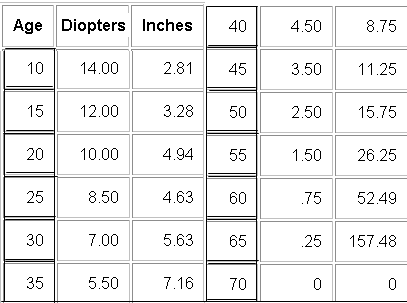
According
to these depressing figures one must expect at thirty to have lost no
less than half of one's original accommodative power, while at forty
two-thirds of it would be gone, and at sixty it would be practically
nonexistent.
There
are many people, however, who do not fit this schedule. Many persons
at forty can read fine print at four inches, although they ought,
according to the table, to have lost that power shortly after
twenty. Worse still, there are people who refuse to become
presbyopic at all. Oliver Wendell Holmes mentions one of these cases
in "The Autocrat of the Breakfast Table."
"There
is now living in New York State," he says, "an old
gentleman who, perceiving his sight to fail, immediately took to
exercising it on the finest print, and in this way fairly bullied
Nature out of her foolish habit of taking liberties at
five-and-forty, or thereabout. And now this old gentleman performs
the most extraordinary feats with his pen, showing that his eyes must
be a pair of microscopes. I should be afraid to say how much he
writes in the compass of a half-dime - whether the Psalms or the
Gospels, or the Psalms and the Gospels, I won't be positive."
(9)
There
are also people who regain their near vision after having lost it for
ten, fifteen, or more years; and there are people who, while
presbyopic for some objects, have perfect sight for others. Many
dressmakers, for instance, can thread a needle with the naked
eye, and with the retinoscope it can be demonstrated that
they accurately focus their eyes upon such objects; and yet they
cannot read or write without glasses.
So
far as I am aware no one but myself has ever observed the
last-mentioned class of cases, but the others are known to every
ophthalmologist of any experience. One hears of them at the meetings
of ophthalmological societies; they are even reported in the medical
journals; but such is the force of authority that when it comes
to writing books they are either ignored or explained away, and every
new
treatise
that comes from the press repeats the old superstition that
presbyopia is "a normal result of growing old." We have
beaten Germany; but the dead hand of German science still oppresses
our intellects and prevents us from crediting the plainest evidence
of our senses. Some of us are so filled with repugnance for the
Hun that we can no longer endure the music of Bach, or the language
of Goethe and Schiller; but German ophthalmology is still
sacred, and no facts are allowed to cast discredit upon it.
Fortunately
for those who feel called upon to defend the old theories,
myopia postpones the advent of presbyopia. and a decrease in the size
of the pupil, which often takes place in old age, has some effect in
facilitating vision at the near-point.
Reported
cases of persons reading without glasses when over fifty or
fifty-five years of age, therefore, can be easily disposed of by
assuming that the subjects must be myopic, or that their pupils are
unusually small. If the case comes under actual observation,
the matter may not be so simple, because it may be found that the
patient, so far from being myopic, is hypermetropic, or emmetropic,
and that the pupil is of normal size. There is nothing to da with
these cases but to ignore them. Abnormal changes in the form of
the lens have also been held responsible for the retention of
near vision beyond the prescribed age, or for its restoration after
it has been lost, the swelling of the lens in incipient cataract
affording a very convenient and plausible explanation for the latter
class of cases. In cases of premature presbyopia "accelerated
sclerosis" (10) Of the lens and weakness of the ciliary muscle
have been assumed; and if such cases as the dressmakers who can
thread their needles when they can no longer read the newspapers
had been observed, no doubt some explanation consistent with the
German viewpoint would have been found for them.
The
truth about presbyopia is that it is not "a normal result
of growing old," being both preventable and curable. It is not
caused by hardening of the lens, but by a strain to see at the
near-point. It has no necessary connection with age, since it occurs,
in
some
cases, as early as ten years, while in others it never occurs at all,
although the subject may live far into the so-called presbyopic age.
It is true that the lens does harden with advancing years, just as
the bones harden and the structure of the skin changes; but since the
lens is not a factor in accommodation, this fact is immaterial, and
while in some cases the lens may become flatter, or lose some of its
refractive power with advancing years, it has been observed
to remain perfectly clear and unchanged in shape up to the age of
ninety. Since the ciliary muscle is also not a factor in
accommodation, its weakness or atrophy can contribute nothing to the
decline of accommodative power. Presbyopia is, in fact, simply a form
of hypermetropia in which the vision for the near-point is chiefly
affected, although the vision for the distance, contrary to what
is generally believed, is always lowered also. The difference between
the two conditions is not always clear. A person with hypermetropia
may or may not read fine print, and a person at the presbyopic
age may read it without apparent inconvenience and yet have
imperfect sight for the distance. In both conditions the sight at
both points is lowered, although the patient may not be aware of
it.
It
has been shown that when the eyes strain to see at the near-point the
focus is always pushed farther away than it was before, in one or all
meridians; and by means of simultaneous retinoscopy it can always be
demonstrated that when a person with presbyopia tries
to read fine print and fails, the focus is always pushed farther away
than it was before the attempt was made, indicating that the failure
was caused by strain. Even the thought of making such an effort will
produce strain, so that the refraction may be changed, and pain,
discomfort and fatigue produced, before the fine print is regarded.
Furthermore,
when a person with presbyopia rests the eyes by closing them, or
palming, he always becomes able, for a few moments at least, to read
fine print at six inches, again indicating that his previous failure
was due, not to any fault of the eyes, but to a strain to see. When
the strain is
permanently
relieved the presbyopia is permanently cured, and this has happened,
not in a few cases, but in many, and at all ages, up to sixty,
seventy and eighty.
The
first patient that I cured of presbyopia was myself. Having
demonstrated by means of experiments on the eyes of animals that
the lens is not a factor in accommodation, I knew that presbyopia
must be curable, and I realized that I could not look for any very
general acceptance of the revolutionary conclusions I had reached so
long as I wore glasses myself for a condition supposed to be due to
the loss of the accommodative power of the lens. I was then suffering
from the maximum degree of presbyopia. I had no accommodative
power whatever, and had to have quite an outfit of glasses, because
with a glass, for instance, which enabled me to read fine print at
thirteen inches, I could not read it either at twelve inches or at
fourteen. The retinoscope shows that when I tried to see anything at
the near-point without glasses my eyes were focussed for the
distance, and when I tried to see anything at the distance
they were focussed for the near-point. My problem, then, was to find
some way of reversing this condition and inducing my eyes to focus
for the point I wished to see at the moment that I wished to see it.
I consulted various eye specialists, but my language was to them like
that of St. Paul to the Greeks, namely, foolishness. "Your lens
is as hard as a stone," they said. "No one can do anything
for you." Then I went to a nerve specialist. He used the
retinoscope on me, and confirmed my own observations as to the
peculiar contrariness of my accommodation; but he had no idea
what I could do about it.
He
would consult some of his colleagues, he said, and asked me to come
back in a month, which I did. Then he told me he had come to the
conclusion that there was only one man who could cure me, and that
was Dr. William H. Bates of New York.
"Why
do you say that?" I asked.
"Because
you are the only man who seems to know anything about it," he
answered.
Thus
thrown upon my own resources, I was fortunate enough to find a
non-medical gentleman who was willing to do what he could to assist
me, the Rev. R. B. B. Foote, of Brooklyn. He kindly used the
retinoscope through many long and tedious hours while I studied my
own case, and tried to find some way of accommodating when I wanted
to read, instead of when I wanted to see something at the distance.
One
day, while looking at a picture of the Rock of Gibraltar which hung
on the wall, I noted some black spots on its face. I imagined that
these spots were the openings of caves, and that there were people in
these caves moving about. When I did this my eyes were focussed for
the reading distance. Then I looked at the same picture at the
reading distance, still imagining that the spots were caves with
people in them. The retinoscope showed that I had accommodated,
and I was able to read the lettering beside the picture. I had, in
fact, been temporarily cured by the use of my imagination.
Later
I found that when I imagined the letters black I was able to see them
black, and when I saw them black I was able to distinguish their
form. My progress after this was not what could be called rapid. It
was six months before I could read the newspapers with any kind of
comfort, and a year before I obtained my present accommodative range
of fourteen inches, from four inches to eighteen; but the experience
was extremely valuable, for I had in pronounced form every symptom
subsequently observed in other presbyopic patients.
Fortunately
for the patients, it has seldom taken me as long to cure other people
as it did to cure myself. In some cases a complete and permanent cure
was effected in a few minutes. Why, I do not know. I will never be
satisfied till I find out. A patient who had worn glasses for
presbyopia for about twenty years was cured in less than fifteen
minutes by the use of his imagination.
When
asked to read diamond type, he said he could not do so, because the
letters were grey and looked
all
alike. I reminded him that the type was printer's ink and that there
was nothing blacker than printer's ink. I asked him if he had
ever seen printer's ink. He replied that he had. Did he remember how
black it was? Yes. Did he believe that these letters were as black as
the ink he remembered? He did, and then he read the letters; and
because the improvement in his vision was permanent, he said
that I had hypnotized him.
In
another case a presbyope of ten years' standing was cured just as
quickly by the same method. When reminded that the letters which he
could not read were black, he replied that he knew they were black,
but that they looked grey.
"If
you know they are black, and yet see them grey," I said, "you
must imagine them grey. Suppose you imagine that they are black. Can
you do that ?"
"Yes,"
he said, "I can imagine that they are black"; and then he
proceeded to read them.
These
extremely quick cures are rare. In nine cases out of ten progress has
been much slower, and it has been necessary to resort to all the
methods of obtaining relaxation found useful in the treatment of
other errors of refraction. In the more difficult cases of presbyopia
the patients often suffer from the same illusions of color, size,
form and number, when they try to read fine print, as do patients
with hypermetropia, astigmatism, and myopia when they try to read the
letters on the Snellen test card at the distance. They are unable to
remember or imagine, when trying to see at the near-point, even
such a simple thing as a small black spot, but can remember it
perfectly when they do not try to see. Their sight for the distance
is often very imperfect and always below normal, although they may
have thought it perfect; and just as in the case of other errors of
refraction, improvement of the distant vision improves the vision at
the near-point.
Regardless,
however, of the difficulty of the case and the age of the patient;
some improvement has always been obtained, and if the treatment was
continued long enough, the patient has been cured.
The
idea that presbyopia is "a normal result of growing old" is
responsible for much defective eyesight. When people who have reached
the presbyopic age experience difficulty in reading, they are very
likely to resort at once to glasses, either with or without
professional advice. In some cases such persons may be actually
presbyopic; in others the difficulty may be something temporary,
which they would have thought little about if they had been younger,
and which would have passed away if Nature had been left to herself.
But once the glasses are adopted, in the great majority of cases,
they produce the condition they were designed to relieve, or, if it
already existed, they make it worse, sometimes very rapidly, as every
ophthalmologist knows. In a couple of weeks sometimes, the patient
finds, as noted in the chapter on What Glasses Do to Us, that the
large print which he could read without difficulty before he got his
glasses, can no longer be read without their aid.
In
from five to ten years the accommodative power of the eye is usually
gone; and if from this point the patient does not go on to cataract,
glaucoma, or inflammation of the retina, he may consider himself
fortunate. Only occasionally do the eyes refuse to submit to the
artificial conditions imposed upon them; but in such cases they may
keep up an astonishing struggle against them for long periods. A
woman of seventy, who had worn glasses for twenty years, was still
able to read diamond type and had good vision for the distance
without them. She said the glasses tired her eyes and blurred her
vision, but that she had persisted in wearing them, in spite of a
continual temptation to throw them off, because she had been
told that it was necessary for her to do so.
If
persons who find themselves getting presbyopic, or who have arrived
at the presbyopic age, would, instead of resorting to glasses, follow
the example of the gentleman mentioned by Dr. Holmes, and make a
practice of reading the finest print they can find, the idea that the
decline of accommodative power is "a normal result of growing
old" would soon die a natural death.
CITATIONS
1.
On the Anomalies of Accommodation and Refraction of the Eye, p.
223.
2.
Roosa: A Clinical Manual of Diseases of the Eye, 1894, p. 537;
Oliver: System of Diseases of the Eye, vol. iv, p, 431.
3.
On the Anomalies of Accommodation and Refraction of the Eye, p. 210.
4.
Diseases of the Eye, p. 148.
5.
Text-book of Ophthalmology, authorized translation from the twelfth
German edition by Duane, 1919, p. 862. Ernst Fuchs (1851- ).
Professor of Ophthalmology at Vienna from 1885 to 1915. His Text-book
of Ophthalmology has been translated into many languages.
6.
A Clinical Manual of Diseases of the Eye, p. 535.
7.
Vol. i, p. 504.
8.
An eye which, when it is at rest, focusses parallel rays upon the
retina, is said to be emmetropic or normal.
9.
Everyman's Library, 1908, pp. 166-167.
10.
Fuchs: Text-book of Ophthalmology, p. S05.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXI
SQUINT AND AMBLYOPIA - THEIR CAUSE
Since
we have two eyes, it is obvious that in the act of sight two pictures
must be formed; and in order that these two-pictures shall be fused
into one by the mind, it is necessary that there shall be perfect
harmony of action between the two organs of vision. In looking at a
distant object the two visual axes must be parallel, and in looking
at an object at a less distance than infinity, which for practical
purposes is less than twenty feet, they must converge to exactly the
same degree. The absence of this harmony of action is known as
squint, or strabismus and is one of the most distressing of eye
defects, not only because of the lowering of vision involved, but
because the want of symmetry in the most expressive feature of
the face which results from it has a most unpleasant effect upon the
personal appearance. The condition is one which has long baffled
ophthalmological science. While the theories as to its cause advanced
in the text-books seem to fit some cases, they leave others
unexplained, and all methods of treatment are admitted to be very
uncertain in their results.
The
idea that a lack of harmony in the movements of the eye is due to a
corresponding lack of harmony in the strength of the muscles that
turn them in their sockets seems such a natural one that this theory
was almost universally accepted at one time.
Operations
based upon it once had a great vogue; but to-day they are advised, by
most authorities, only as a last resort. It is true that many persons
have benefited by them; but at best the correction of the squint is
only approximate, and in many cases the condition has been made
worse, while a restoration of binocular vision - the power of fusing
the two visual images into one - is scarcely even hoped for.(1)
The
muscle theory fitted the facts so badly that when Donders advanced
the idea that squint was a condition growing out of refractive errors
- hypermetropia being held responsible for the production of
convergent and myopia for divergent squint - it was universally
accepted. This theory, too, proved unsatisfactory, and now medical
opinion is divided between various theories. Hansen-Grut attributed
the condition, in the great majority of cases, to a defect, not of
the muscles, but of the nerve supply; and this idea has had many
supporters. Worth and his disciples lay stress on the lack of a
so-called fusion faculty, and have recommended the use of prisms, or
other measures, to develop it. Stevens believes that the anomaly
results from a wrong shape of the orbit, and as it is impossible to
alter this condition, advocates operations for the purpose of
neutralizing its influence.
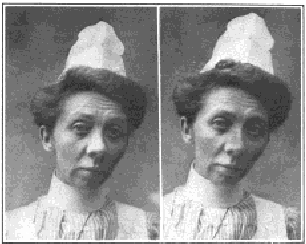
Fig.
53 -- No. 1. - Reading the Snellen test card with normal
vision; visual axes parallel.
No.
2. - The same patient making an effort to see the test card;
myopia and convergent squint of the left eye have been produced.
In
order to make any of these theories appear consistent it is necessary
to explain away a great many troublesome facts. The uncertain result
of operations upon the eye muscles is sufficient to cast suspicion on
the theory that the condition is due to any abnormality of the
muscles, and many cases of marked paralysis of one or more muscles
have been
observed
in which there was no squint. Relief of paralysis, moreover, may not
relieve the squint, nor the relief of the squint the paralysis. Worth
found so many cases which were not benefited by training designed to
improve the fusion faculty that he recommended operations on the
muscles in such cases; while Donders, noting that the majority of
hypermetropes did not squint, was obliged to assume that
hypermetropia did not cause this condition without the aid of
co-operating circumstances.
That
the state of the vision is not an important factor in the
production of squint is attested by a multitude of facts. It is
true, as Donders observed, that squint is usually associated with
errors of refraction; but some people squint with a very slight
error of refraction. It is also true that many persons with
convergent squint have hypermetropia; but many others have not. Some
persons with convergent squint have myopia. A person may
also have convergent squint with one eye normal and one
hypermetropic or myopic, or with one eye blind. Usually the
vision of the eye that turns in is less than that of the eye which is
straight; yet there are cases in which the eye with the poorer vision
is straight and the eye with the better vision turned in. With two
blind eyes, both eyes may be straight, or one may turn in. With one
good eye and one blind eye, both eyes may be straight. The blinder
the eye, as a rule, the more marked the squint; but exceptions
are frequent, and in rare cases an eye with nearly normal vision
may turn in persistently. A squint may disappear and return
again, while convergent squint will change into divergent squint
and back again. With the same error of refraction, one person will
have squint and the other not. A third will squint with a different
eye. A fourth will squint first with one eye and then with the other.
In a fifth the amount of the squint will vary. One will get well
without glasses, or other treatment, and another with these
things. These cures may be temporary, or permanent, and the
relapses may occur either with or without glasses.
However
slight the error of refraction, the vision of many squinting eyes is
inferior to that of the straight eye, and for this condition,
usually, no apparent or sufficient cause can be found in the
constitution of the eye. There is a difference of opinion as to
whether this curious defect of vision is the result of the squint, or
the squint the result of the defect of vision; but the predominating
opinion that it is, at least, aggravated by the squint has been
crystallized in the name given to the condition, namely, amblyopia ex
anopsia, literally dim-sightedness from non-use - for in order
to avoid the annoyance of double vision the mind is believed to
suppress the image of the deviating eye. There are, however,
many squinting eyes without amblyopia, while such a condition has
been found in eyes that have never squinted.
The
literature of the subject is full of the impossibility of curing
amblyopia, and in popular writings persons having the care of
children are urged to have cases of squint treated early, so that the
vision of the squinting eye may not be lost. According to Worth, not
much improvement can ordinarily be obtained in amblyopic eyes
after the age of six, while Fuchs says,(2) "The function of the
retina never again becomes perfectly normal, even if the cause of the
visual disturbance is done away with." Yet it is well known, as
the translator of Fuchs points out in an editorial comment upon the
above statement,(3) that if the sight of the good eye is lost at any
period of life, the vision of the amblyopic eye will often become
normal.
Furthermore,
an eye may be amblyopic at one time and not at another. When the good
eye is covered a squinting eye may be so amblyopic that it can
scarcely distinguish daylight from darkness; but when both eyes
are open, the vision of the squinting eye may be found to be as good
as that of the straight eye, if not better. In many cases, too, the
amblyopia will change from one eye to the other.
Double
vision occurs very seldom in squint, and when
it
does it often assumes very curious forms. When the eyes turn in the
image seen by the right eye should, according to all the laws of
optics, be to the right, and the image seen by the left eye to the
left. When the eyes turn out the Opposite should be the case. But
often the position of the images is reversed, the image of the
right eye in convergent squint being seen to the left and that of the
left eye to the right, while in divergent squint the opposite is
the case. This condition is known as paradoxical diplopia..
Furthermore, persons with almost normal vision and both eyes
perfectly straight may have both kinds of double vision.
All
the theories heretofore suggested fail to explain the foregoing
facts; but it is a fact that in all cases of squint a strain can be
demonstrated, and that the relief of the strain is in all cases
followed by the cure of the squint, as well as of the amblyopia and
the error of refraction. It is also a fact that all persons with
normal eyes can produce squint by a strain to see. It is not a
difficult thing to do, and many children derive much amusement from
the practice, while it gives their elders unnecessary concern,
for fear the temporary squint may become permanent. To produce
convergent squint is comparatively easy. Children usually
do it by straining to see the end of the nose. The production of
divergent squint is more difficulty, but with practice persons
with normal eyes become able to turn out either eye, or both, at
will. They also become able to turn either eye upward and inward, or
upward and outward, at any desired angle. Any kind of squint can, in
fact, be produced at will by the appropriate kind of strain. Some
persons retain the power to produce voluntary squint more or less
permanently. Others quickly lose it if they do not keep in practice.
There is usually a lowering of the vision when voluntary squint is
produced, and accepted methods of measuring the strength of the
muscles seem to show deficiencies corresponding to the nature of the
squint.
CITATIONS
1.
The result obtained by the operation is, as a rule, simply cosmetic.
The sight of the squinting eye is not influenced by the operation,
and in only a few instances is even binocular vision restored. -
Fuchs: Text-Book of Ophthalmology, p. 795.
The
result of even the most successful squint operation, in
long-standing strabismus, is merely cosmetic in the vast
majority of cases. -
Eversbusch
: The Diseases of Children, edited by Pfaunder and Schlossman.
English translation by Shaw and La Fetra, second edition, 1912-1914,
vol. vii, p. 316.
2.
Text-Book of Ophthalmology, p. 633.
3.
Cases have been reported, some surely authentic, in which an
amblyopic squinting eye has acquired good vision, either through
correction of the refraction, or because loss of sight in the good
eye has compelled the use of the amblyopic eye. - Ibid.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXII
SQUINT AND AMBLYOPIA: THEIR CURE
THE
evidence is conclusive that squint and amblyopia, like errors of
refraction, are purely functional troubles; and since they are always
relieved by the relief of the strain with which they are associated,
it follows that any of the methods which promote relaxation and
central fixation may be employed for their cure. As in the case of
errors of refraction, the squint disappears and the amblyopia is
corrected just as soon as the patient gains sufficient mental control
to remember a perfectly black period. In this way both conditions can
be temporarily relieved in a few seconds, their permanent cure being
a mere matter of making this temporary state permanent.
One
of the best ways of gaining mental control in cases of squint is to
learn how to increase the squint, or produce other kinds of squint,
voluntarily.
In
the case illustrated the patient had divergent vertical squint in
both eyes. When the left eye was straight the right eye turned out
and up, and when the right eye was straight the left eye turned down
and out. Both eyes were amblyopic and there was double vision, with
the images sometimes on the same side and sometimes on opposite
sides.
The
patient suffered from headaches, and having obtained no relief
from glasses, or other methods of treatment, she made up her mind to
an operation and consulted Dr. Gudmund J. Gislason, of Grand Forks,
N. D., with a view to having one performed.
Dr.
Gislason, puzzled to find so many muscles apparently at fault,
asked my opinion as to which of them should be operated upon. I
showed the patient how to make her squint worse, and recommended that
Dr. Gislason treat her by eye education without an operation. He did
so, and in less than a month the patient had learned to turn both
eyes in voluntarily.
At
first she did this by looking at a pencil held over the bridge of the
nose; but later she became able to do it without the pencil, and
ultimately she became able to produce every kind of squint at will.
The treatment was not pleasant for her, because the production of new
kinds of squint, or the making worse of the existing condition, gave
her pain; but it effected a complete and permanent cure both of the
squint and of the amblyopia. The same method has proved successful
with other patients.
Some
patients do not know whether they are looking straight at an object
or not. These may be helped by watching the deviating eye and
directing them to look more nearly in the proper direction. When the
deviating eye looks directly at an object the strain to see is less,
and the vision is consequently improved. Covering the good eye
with an opaque screen, or with ground glass, encourages a more proper
use of the squinting eye, especially if the vision of that eye is
imperfect.
Children
of six years, or younger, can usually be cured of squint by the use
of atropine, a one per cent solution being instilled into one or both
eyes twice a day, for many months, a year, or longer. The atropine
makes it more difficult for the child to see, and makes the sunlight
disagreeable. In order to overcome this handicap it has to relax, and
the relaxation cures the squint.
The
improvement resulting from eye education in cases of squint and
amblyopia is sometimes so rapid as to be almost incredible. The
following are a few of many other examples that might be quoted:
Fig.
54. Case of Divergent Vertical Squint Cured by Eye Education
--No. 1. - The right eye turns out and up, the left being straight.
No. 2. - The patient learns to look down and out with the left eye
while the right looks staring.
No.
3. - The patient learns to turn both eyes in by looking at a pencil
held over the bridge of the nose. No. 4. - The patient is permanently
cured. All four pictures were taken within fifteen minutes of each
other, the patient having learned to reproduce the conditions
represented at will.
A
girl of eleven had convergent vertical squint of the left eye. The
vision of this eye at the distance was 3/200, while at the near-point
it was so imperfect that she was unable to read. The vision of the
right eye was normal both for the near-point and the distance. She
was wearing glasses when she came to the office - convex 4.00 D. S.
combined with convex 0.50 D. C., axis 90, for the right eye; and
convex 5.50 D. S. for the left eye - but had obtained no benefit from
them. When she looked three feet away from the big C with the left
eye, she saw it better than when she looked directly at it; but when
asked to count my fingers held three feet away from the card, they so
attracted her attention that she was able to see the large letter
worse. The fact was impressed upon her that she could see the card
better when she looked away from it, or she could see it worse, at
will; and she was also asked to note that when she saw it worse her
vision improved, and when she saw it better her vision declined.
After shifting from the card to a point three feet away from it, and
seeing the former worse a few times, her vision improved to 10/200.
The ability to shift and see worse improved by practice so rapidly
that in less than ten days her vision was normal in both eyes, and in
less than two weeks it had improved to 20/10, while diamond type was
read with each eye at from three inches to twenty inches. In less
than three weeks her vision for the distance was 20/5, by artificial
light, and she read photographic type reductions at two inches,
the tests being made with both eyes together and with each eye
separately She also read strange test cards as readily as the
familiar ones. She was advised to continue the treatment at home to
prevent a relapse, and at the end of three years none had occurred.
During the treatment at the office and practice at home the good eye
was covered with an opaque screen, but this was not worn at other
times.
A
very remarkable case was that of a girl of fourteen who had
squinted from childhood. The internal rectus of the right eye had
been cut when she was two years old, but still pulled the eye inward.
The patient objected to wearing a ground glass over her good eye,
because her friends teased her about it and she thought it made her
more conspicuous than the squint. One day she lost her glasses in the
snow; but her father, who was a man of strong character, immediately
provided another pair. Then she announced that she was ill, and
couldn't go to school. I told the father that his daughter was
hysterical, and simply imagined she was ill to avoid treatment. He
insisted that she continue, and as she did not consider herself well
enough to come to see me, I called upon her. With the assistance of
her father she was made to understand that she would have to continue
the treatment until she was cured, and she at once went to work with
such energy and intelligence that in half an hour the vision of
the squinting and amblyopic eye had improved from 3/200 to 20/30. She
also became able to read fine print at twelve inches. She went back
to school wearing the ground glass over the good eye; but whenever
she wanted to see she looked over the top of it. Her father followed
her to school, and insisted that she use the poorer eye instead of
the better one. She became convinced that the simplest way out of her
troubles would be to follow my instructions, and in less than a week
the squint was corrected and she had perfect vision in both eyes. At
the beginning of the treatment she could not count her fingers at
three feet with the poorer eye, and in three weeks, including all the
time that she wasted, she had perfect sight. When told that she
was cured her main concern seemed to be to know whether she would
have to wear the ground glass any more. She was assured that she
would not have to do so unless there was a relapse, but there never
was any relapse.(1)
A
girl of eight had had amblyopia and squint since childhood. The
vision of the right eye was 10/40, while that of the left was 20/30.
Glasses did not improve either eye. The patient was seated twenty
feet from a Snellen test card and the right, or poorer eye, was
covered with an opaque screen. She was directed to look with her
better eye at the large letter on the card and to note its clearness.
Next she was told to look at a point three feet to one side of the
card, and her attention was called to the fact that she did not then
see the large letter so well. The point of fixation was brought
closer and closer to the letter, until she appreciated the fact that
her vision was lowered when she looked only a few inches to one side
of it. When she looked at a small letter she readily recognized that
an eccentric fixation of less than an inch lowered the vision.
After
she had learned to increase the amblyopia of the better eye, this eye
was covered while she was taught how to lower the vision of the
other, or poorer eye, by increasing its eccentric fixation. This
was accomplished in a few minutes. She was told that the cause of her
defective sight was her habit of looking at objects with a part of
the retina to one side of the true center of sight. She was advised
to see by looking straight at the Snellen card. In less than half an
hour the vision of the left eye became normal, while the right
improved from 10/l40 to 10/10. The cure was complete in two weeks.
The
following case was unusually prolonged, because as soon as one eye
had been cured the defect for which it had been treated appeared in
the other eye. The patient, a child of ten, had imperfect sight in
both eyes, but worse in the right than in the left. The vision of the
right eye was restored after some weeks by eye education, when the
left eye turned in and became amblyopic. The right eye was then
covered, and after a few weeks of eye education the left became
normal. The right eye then turned in and the vision became defective.
It was necessary
to
educate the eyes alternately, for about a year, before both became
normal at the same time. This patient had congenital paralysis of the
external rectus muscle in both eyes, a condition which was apparently
not relieved when the squint and amblyopia were cured.

Fig.
55 -- No. 1. - Convergent squint of the right eye.
No.
2. - The patient is temporarily cured by the memory of a black
period.
In
the following case the patient had an attack of infantile paralysis
after her cure, resulting in a relapse, with new and more
serious developments, which were, however, quickly cured. The
patient, a girl of six, seen first on December 11, 1914, had had
divergent squint of the left eye for three years, and had worn
glasses for two years without benefit - convex 2.50 D. S. for the
right eye, and convex 6.00 D. S. combined with convex 1.00 D. C.,
axis 90, for the left The vision of the right eye with glasses was
12/15 and of the left 12/200. Atropine was prescribed for the
right eye for the purpose of partially blinding it and thus
encouraging a more nearly proper use of the squinting eye, and the
usual methods of securing relaxation, such as shifting, palming,
the exercise of the memory, etc., were used. On January 13, 1915, the
vision without glasses had improved to 10/70 for the right eye,
and 10/50 for the left. On February 6, the vision of the right eye
was 10/40 and of the left 10/30. The eyes were apparently straight,
and scientific tests showed that both were used at the same time
(binocular
single
vision). On April 17, after about four months' treatment, the vision
of the left eye was normal, and there was binocular single vision at
six inches. On May 1 the vision of the left eye was still normal, and
whereas at the beginning the patient had been unable to read
with it at all, even with glasses, she now read diamond type without
glasses at six inches.
On
August 16, 1916, the patient had an attack of infantile paralysis
which was then epidemic. The sight of both eyes failed, the muscles
that turned the eyes in and out were paralyzed, the eyelids twitched,
and there was double vision. Various muscles of the head, the
left leg and the left arm were also paralyzed. When she left the
hospital after five weeks the left eye was turned in, and the vision
of both eyes was so poor that she was unable to recognize her
mother. Later she developed alternate convergent squint. On November
2 the paralysis in the right eye subsided, and four weeks later that
of the left eye began to improve. On November 9 she returned for
treatment without any conspicuous squint, but still suffering from
double vision, with the images sometimes on the same side and
sometimes on opposite sides. On November 23 the eyes were
straight and the vision normal.
On
July 11, 1918, the eyes were still straight and the vision normal,
and there was binocular single vision at six inches. Although
atropine had been used in the right eye every day for more than a
year, and intermittently for a much longer time, and the pupil was
dilated to the maximum, it read fine print without difficulty at
six inches, central fixation overcoming the paralyzing
effect of the drug. According to the current theory the accommodation
should have been completely paralyzed, making near vision quite
impossible. The patient also read fine print with the left eye as
well as, or better than, with the right eye.
CITATIONS
Bates:
L'education de l'oeil dans líamblyopie ex anopsia, Clin.
Opht., Dec. 10, 1912.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXIII
FLOATING SPECKS: THEIR CAUSE AND CURE
A
very common phenomenon of imperfect sight is the one known to medical
science as muscae volitantes or flying flies. These floating
specks are usually dark or black, but sometimes appear like white
bubbles, and in rare cases may assume all the colors of the
rainbow. They move somewhat rapidly, usually in curving lines, before
the eyes, and always appear to be just beyond the point of fixation.
If one tries to look at them directly, they seem to move a little
farther away. Hence their name of "flying flies."
The
literature of the subject is full of speculations as to the origin of
these appearances. Some have attributed them to the presence of
floating specks - dead cells, or the debris of cells - in the
vitreous humor, the transparent substance that fills four-fifths of
the eyeball behind the crystalline lens.
Similar
specks on the surface of the cornea have also been held responsible
for them. It has even been surmised that they might be caused by the
passage of tears over the cornea. They are so common in myopia
that they have been supposed to be one of the symptoms of this
condition, although they occur also with other errors of refraction,
as well as in eyes otherwise normal. They have been attributed to
disturbances of the circulation, the digestion and the kidneys, and
because so many insane people have them, have been thought to be an
evidence of incipient insanity. The patent-medicine business has
thrived upon them, and it would be difficult to estimate the
amount of mental torture they cause, as the following cases
illustrate.
A
clergyman who was much annoyed by the continual appearance of
floating specks before his eyes was told by his eye specialist that
they were a symptom of kidney disease, and that in many cases of
kidney trouble disease of the retina might be an early symptom.
So at regular intervals he went to the specialist to have his
eyes examined, and when at length the latter died, he looked around
immediately for some one else to make the periodical examination.
His
family physician directed him to me. I was by no means so well known
as his previous ophthalmological adviser, but it happened that I had
taught the family physician how to use the ophthalmoscope after
others had failed to do so. He thought, therefore, that I must
know a lot about the use of the instrument, and what the
clergyman particularly wanted was some one capable of making a
thorough examination of the interior of his eyes and
detecting at once any signs of kidney disease that might make their
appearance. So he came to me, and at least four times a year for ten
years he continued to come.
Each
time I made a very careful examination of his eyes, taking as much
time over it as possible, so that he would believe that it was
careful; and each time he went away happy because I could find
nothing wrong. Once when I was out of town he got a cinder in his
eye, and went to another oculist to get it out. When I came back late
at night I found him sitting on my door step, on the chance that I
might return. His story was a pitiable one. The strange doctor had
examined his eyes with the ophthalmoscope, and had suggested the
possibility of glaucoma, describing the disease as a very treacherous
one which might cause him to go suddenly blind and would be
agonizingly painful. He emphasized what the patient had
previously been told about the danger of kidney disease, suggested
that the liver and heart might also be involved, and advised him to
have all of these organs carefully examined. I made another
examination of his eyes in general and their tension in
particular; I had him feel his eyeballs and compare them
with my own, so that he might see for himself that they were not
becoming hard as a stone; and finally I succeeded in reassuring him.
I have no doubt, however, that he went at once to his family
physician for an examination of his internal organs.
A
man returning from Europe was looking at some white clouds one day
when floating specks appeared before his eyes. He consulted the
ship's doctor, who told him that the symptom was very serious, and
might be the forerunner of blindness. It might also indicate
incipient insanity, as well as other nervous or organic diseases. He
advised him to consult his family physician and an eye specialist as
soon as he landed, which he did. This was twenty-five years ago, but
I shall never forget the terrible state of nervousness and terror
into which the patient had worked himself by the time he came to me.
It was even worse than that of the clergyman, who was always ready to
admit that his fears were unreasonable. I examined his eyes very
carefully, and found them absolutely normal. The vision was perfect
both for the near-point and the distance. The color perception, the
fields and the tension were normal; and under a strong magnifying
glass I could find no opacities in the vitreous. In short, there were
absolutely no symptoms of any disease. I told the patient there was
nothing wrong with his eyes, and I also showed him an advertisement
of a quack medicine in a newspaper which gave a great deal of space
to describing the dreadful things likely to follow the appearance of
floating specks before the eyes, unless you began betimes to take the
medicine in question at one dollar a bottle. I pointed out that the
advertisement, which was appearing in all the big newspapers of the
city every day, and probably in other cities, must have cost a lot of
money, and must, therefore, be bringing in a lot of money.
Evidently
there must be a great many people suffering from this symptom,
and if it were as serious as was generally believed, there would be a
great many more blind and insane people in the community than there
were. The patient went away somewhat comforted, but at eleven
o'clock - his first visit had been at nine - he was back again. He
still saw the floating specks, and was still worried about them. I
examined his eyes again as carefully as before, and again was able to
assure him that there was nothing wrong with them. In the afternoon I
was not in my office, but I was told that he was there at three and
at five. At seven he came again, bringing with him his family
physician, an old friend of mine. I said to the latter: "Please
make this patient stay at home. I have to charge him for his visits,
because he is taking up so much of my time; but it is a shame to take
his money when there is nothing wrong with him."
What
my friend said to him I don't know, but he did not come back again.
I
did not know as much about muscae volitantes then as I know now, or I
might have saved both of these patients a great deal of uneasiness. I
could tell them that their eyes were normal, but I did not know how
to relieve them of the symptom, which is simply an illusion resulting
from mental strain. The specks are associated to a considerable
extent with markedly imperfect eyesight, because persons whose
eyesight is imperfect always strain to see; but persons whose
eyesight is ordinarily normal may see them at times, because no eye
has normal sight all the time. Most people can see muscae volitantes
when they look at the sun, or any uniformly bright surface, like a
sheet of white paper upon which the sun is shining. This is because
most people strain when they look at surfaces of this kind. The
specks are never seen, in short, except when the eyes and mind are
under a strain, and they always disappear when the strain is
relieved. If one can remember a small letter on the Snellen test card
by central fixation, the specks will immediately disappear, or cease
to move; but if one tries to remember two or more letters equally
well at one time, they will reappear and move.
Usually
the strain that causes muscae volitantes is very easily relieved. A
school teacher who had been annoyed by these appearances for years
came to me because the condition had grown recently much worse. I was
able in half an hour to improve her sight, which had been slightly
myopic, to normal, whereupon the specks disappeared. Next day they
came back, but another visit to the office brought relief. After that
the patient was able to carry out the treatment at home, and had no
more trouble.
A
physician who suffered constantly from headaches and muscae
volitantes was able to read only 20/70 when he looked at the Snellen
test card, while the retinoscope showed mixed astigmatism and he saw
the specks.
When
he looked at a blank wall, or a blank white card, the retinoscope
still showed mixed astigmatism and he still saw the specks.
When, however, he remembered a black spot as well as he could see it,
when looking at these surfaces. there were no specks, and the
retinoscope indicated no error of refraction. In a few days he
obtained complete relief from the astigmatism, the muscae volitantes,
and the headaches, as well as from chronic conjunctivitis. His
eyes, which had been partly closed, opened wide, and the sclera
became white and clear. He became able to read in moving trains with
no inconvenience, and - what impressed him more than anything else -
he also became able to sit up all night with patients without having
any trouble with his eyes next day.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXIV
HOME TREATMENT
It
is not always possible for patients to go to a competent
physician for relief. As the method of treating eye defects
presented in this book is new, it may be impossible to find a
physician in the neighborhood who understands it; and the patient may
not be able to afford the expense of a long journey, or to take the
time for treatment away from home. To such persons I wish to say that
it is possible for a large number of people to be cured of defective
eyesight without the aid, either of a physician or of anyone else.
They can cure themselves, and for this purpose it is not necessary
that they should understand all that has been written in this book,
or in any other book. All that is necessary is to follow a few simple
directions.
Place
a Snellen test card on the wall at a distance of ten, fourteen, or
twenty feet, and devote half a minute a day, or longer, to
reading the smallest letters you can see, with each eye separately,
covering the other with the palm of the hand in such a way as to
avoid touching the eyeball. Keep a record of the progress made, with
the dates. The simplest way to do this is by the method used by
oculists, who record the vision in the form of a fraction, with the
distance at which the letter is read as the numerator and the
distance at which it ought to be read as the denominator. The figures
above, or to one side of, the lines of letters on the test card
indicate the distance at which these letters should be read by
persons with normal eyesight. Thus a vision of 10/200 would mean that
the big C, which ought to be read at 200 feet, cannot be seen at a
greater distance than ten feet. A vision of 20/10 would mean
that the ten line, which the normal eye is not ordinarily
expected to read at a greater distance than ten feet, is seen at
double that distance. This is a
standard
commonly attained by persons who have practiced my methods.
Another
and even better way to test the sight is to compare the blackness of
the letter at the near-point and at the distance, in a dim light and
in a good one. With perfect sight, black is not altered by
illumination or distance. It appears just as black at the distance as
at the near-point, and just as black in a dim light as in a good one.
If it does not appear equally black to you under all these
conditions, therefore, you may know that your sight is
imperfect.
Children
under twelve years who have not worn glasses are usually cured of
defective eyesight by the above method in three months, six months,
or a year. Adults who have never worn glasses are benefited in a
very short time -- a week or two -- and if the trouble is not very
bad, may be cured in the course of from three to six months. Children
or adults who have worn glasses, however, are more difficult to
relieve, and will usually have to practice the methods of gaining
relaxation described in other chapters; they will also have to devote
considerable time to the treatment.
It
is absolutely necessary that the glasses be discarded. No
half-way measures can be tolerated, if a cure is desired. Do not
attempt to wear weaker glasses, and do not wear glasses for
emergencies. Persons who are unable to do without glasses for all
purposes are not likely to be able to cure themselves.
Children
and adults who have worn glasses will have to devote an hour or
longer every day to practice with the test card and the balance of
their time to practice on other objects. It will be well for such
patients to have two test cards, one to be used at the near-point,
where it can be seen best, and the other at ten or twenty feet. The
patient will find it a great help to shift from the near card to the
distant one, as the unconscious memory of the letters seen at the
near-point helps to bring out those seen at the distance.
If
you cannot obtain a test card, you can make one for yourself by
painting black letters of appropriate size on a white card, or on a
piece of white paper. The approximate diameter of these letters,
reading from the top of the card to the bottom is: 35 in., 1 3/4 in.,
1 1/4 in., 7/8 in., 11/16 in., 1/2 in., 3/8 in., 1/4 in., 3/16 in.
If
the patient can secure the aid of some person with normal sight, it
will be a great advantage. In fact, persons whose cases are obstinate
will find it very difficult, if not impossible, to cure themselves
without the aid of a teacher. The teacher, if he is to benefit the
patient, must himself be able to derive benefit from the various
methods recommended. If his vision is 10/10, he must be able to
improve it to 20/10, or more. If he can read fine print at twelve
inches, he must become able to read it at six, or at three inches. He
must also have sufficient control over his visual memory to relieve
and prevent pain. A person who has defective sight, either for the
distance or the near-point, and who cannot remember black well
enough to relieve and prevent pain, will be unable to be of any
material assistance in obstinate cases; and no one will be able to be
of any assistance in the application of any method which he himself
has not used successfully.
Parents
who wish to preserve and improve the eyesight of their children
should encourage them to read the Snellen test card every day. There
should, in fact, be a Snellen test card in every family; for when
properly used it always prevents myopia and other errors of
refraction, always improves the vision, even when this is already
normal, and always benefits functional nervous troubles. Parents
should improve their own eyesight to normal, so that their children
may not imitate wrong methods of using the eyes and will not be
subject to the influence of an atmosphere of strain. They should also
learn the principles of central fixation sufficiently well to relieve
and prevent pain, in order that they may teach their children to do
the same. This practice not only makes it possible to avoid
suffering, but is a great benefit to the general health.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXV
CORRESPONDENCE TREATMENT
Correspondence
treatment is usually regarded as quackery, and it would be manifestly
impossible to treat many diseases in this way. Pneumonia and typhoid,
for instance, could not possibly be treated by correspondence, even
if the physician had a sure cure for these conditions and the mails
were not too slow for the purpose. In the case of most diseases, in
fact, there are serious objections to correspondence
treatment.
But
myopia, hypermetropia and astigmatism are functional conditions,
not organic, as the text-books teach and as I believed myself until I
learned better. Their treatment by correspondence, therefore,
has not the drawbacks that exist in the case of most physical
derangements. One cannot, it is true, fit glasses by correspondence
as well as when the patient is in the office, but even this can be
done, as the following case illustrates.
An
old colored woman in the wilds of Honduras. far removed from any
physician or optician, was unable to read her Bible, and her son, a w
waiter in New York, asked me if I could not do something for her. The
suggestion gave me a distinct shock which I will remember as long as
I live. I had never dreamed of the possibility of prescribing glasses
for anyone I had not seen and I had, besides, some very disquieting
recollections of colored women whom I had tried to fit with glasses
at my clinic.
If
I had so much difficulty in prescribing the proper glasses under
favorable conditions, how could I be expected to fit a patient whom I
could not even see? The waiter was deferentially persistent,
however. He had more faith in my genius than I had, and as his
mother was nearing the end of her life, he was very anxious to
gratify her last wishes. So, like the
unjust
judge of the parable, I yielded at last to his importunity, and wrote
a prescription for convex 3.00 D. S. The young man ordered the
glasses and mailed them to his mother, and by return mail came a very
grateful letter stating that they were perfectly satisfactory.
A
little later the patient wrote that she couldn't see objects at the
distance that were perfectly plain to other people, and asked if some
glasses couldn't be sent that would make her see at the distance as
well as she did at the near-point. This seemed a more difficult
proposition than the first one; but again the son was persistent, and
I myself could not get the old lady out of my mind. So again I
decided to do what I could. The waiter had told me that his mother
had read her Bible long after the age of forty. Therefore I knew she
could not have much hypermetropia, and was probably slightly myopic.
1 knew also that she could not have much astigmatism, for in that
case her sight would always have been noticeably imperfect.
Accordingly
I told her son to ask her to measure very accurately the distance
between her eyes and the point at which she could read her Bible best
with her glasses, and to send me the figures. In due time I received,
not figures, but a piece of string about a quarter of an inch in
diameter and exactly ten inches long. If the patient's vision had
been normal for the distance, I knew that she would have been able to
read her Bible best with her glasses at thirteen inches. The string
showed that at ten inches she had a refraction of four diopters.
Subtracting
from this the three diopters of her reading glasses, I got one
diopter of myopia. I accordingly wrote a prescription for concave
1.00 D. S., and the glasses were ordered and mailed to Honduras. The
acknowledgment was even more grateful than in the case of the first
pair. The patient said that for the first time in her life she was
able to read signs and see other objects at a distance as well as
other people did, and that the whole world looked entirely different
to her.
Would
anyone venture to say that it was unethical for me to try to help
this patient? Would it have been better to leave her in her isolation
without even the consolation of Bible reading? I do not think so.
What I did for her required only an ordinary knowledge of
physiological optics, and if I had failed, I could not have done her
much harm.
In
the case of the treatment of imperfect sight without glasses there
can be even less objection to the correspondence method. It is true
that in most cases progress is more rapid and the results more
certain when the patient can be seen personally; but often this is
impossible, and I see no reason why patients who cannot have the
benefit of personal treatment should be denied such aid as can be
given them by correspondence. I have been treating patients in
this way for years, and often with extraordinary success.
Some
years ago an English gentleman wrote to me that his glasses were very
unsatisfactory. They not only did not give him good sight, but they
increased, instead of lessening, his discomfort. He asked if I could
help him, and since relaxation always relieves discomfort and
improves the vision, I did not believe that I was doing him an injury
in telling him how to rest his eyes. He followed my directions with
such good results that in a short time he obtained perfect sight
for both the distance and the near-point without glasses, and was
completely relieved of his pain. Five years later he wrote me that he
had qualified as a sharpshooter in the army. Did I do wrong in
treating him by correspondence? I do not think so.
After
the United States entered the European war, an officer wrote to me
from the deserts of Arizona that the use of his eyes at the
near-point caused him great discomfort, which glasses did not
relieve, and that the strain had produced granulation of the lids. As
it was impossible for him to come to New York, I undertook to treat
him by correspondence. He improved very rapidly. The inflammation of
the lids was relieved almost immediately, and in about four months he
wrote me that he had read one of my own reprints - by no means a
short one - in a dim light, with no bad after effects; that the glare
of
the
Arizona sun, with the Government thermometer registering 114, did not
annoy him; and that he could read the ten line on the test card at
fifteen feet almost perfectly, while even at twenty feet he was able
to make out most of the letters.
A
third case was that of a forester in the employ of the U. S.
Government. He had myopic astigmatism, and suffered extreme
discomfort, which was not relieved either by glasses or by long
summers in the mountains, where he used his eyes but little for close
work. He was unable to come to New York for treatment, and although I
told him that correspondence treatment was somewhat uncertain,
he said he was willing to risk it. It took three days for his
letters to reach me and another three for my reply to reach him,
and as letters were not always written promptly on either side, he
often did not hear from me more than once in three weeks. Progress
under these conditions was necessarily slow; but his discomfort
was relieved very quickly, and in about ten months his sight had
improved from 20/50 to 20/20.
In
almost every case the treatment of patients coming from a distance is
continued by correspondence after they return to their
homes; and although they do not get on so well as when they are
coming to the office, they usually continue to make progress till
they are cured.
At
the same time it is often very difficult to make patients understand
what they should do when one has to communicate with them entirely by
writing, and probably all would get on better if they could have some
personal treatment. At the present time the number of doctors in
different parts of the United States who understand the treatment of
imperfect sight without glasses is altogether too few, and my efforts
to interest them in the matter have not been very successful.
[NOTE:
Interesting enough, this the final sentence of this paragraph appears
in one of the 1920 editions, but not in another!:] I would
consider it a privilege to treat medical men without a fee, and when
cured they will be able to assist me in the treatment of patients in
their various localities.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXVI
THE PREVENTION OF MYOPIA IN SCHOOLS: METHODS THAT FAILED
No
phase of ophthalmology, not even the problem of accommodation, has
been the subject of so much investigation and discussion as the cause
and prevention of myopia. Since hypermetropia was supposed to be
due to a congenital deformation of the eyeball, and astigmatism,
until recently, was also supposed to be congenital in most cases,
these conditions were not thought to call for any explanation, nor to
admit of any prevention; but myopia appeared to be acquired. It
therefore presented a problem of immense practical importance to
which many eminent men devoted years of labor.
Voluminous
statistics were collected regarding its occurrence, and are still
being collected. The subject has produced libraries of
literature. But very little light is to be gained from the perusal of
this material, and for the most part it leaves the reader with an
impression of hopeless confusion. It is impossible even to
arrive at any conclusion as to the prevalence of the complaint; for
not only has there been no uniformity of standards and methods, but
none of the investigators has taken into account the fact that the
refraction of the eye is not a constant condition, but one which
continually varies. There is no doubt, however, that most children,
when they begin school, are free from this defect, and that both the
number of cases and the degree of the myopia steadily increase as the
educational process progresses. Professor Hermann Cohen, of Breslau,
whose report of his study of the eyes of upwards of 10,000 children
first called general attention to this subject, found scarcely one
per cent of myopia in the village schools, twenty to forty per cent
in the Realschulen, thirty to thirty-five in the gymnasia, and
fifty-three to sixty-four in the professional
schools.
His investigations were repeated in many cities of Europe and
America, and his observations, with some difference in percentages,
everywhere confirmed.
These
conditions were unanimously attributed to the excessive use of the
eyes for near work, though, according to the theory that the lens is
the agent of accommodation, it was a little difficult to see just why
near work should have this effect. On the supposition that
accommodation was effected by an elongation of the eyeball, it would
have been easy to understand why an excessive amount of
accommodation should produce a permanent elongation. But why
should an abnormal demand on the accommodative power of the lens
produce a change, not in the shape of that body, but in that of the
eyeball? Numerous answers to this question have been proposed, but no
one has yet succeeded in finding a satisfactory one. (1) In the case
of children it has been assumed by many authorities that, since the
coats of the eye are softer in youth than in later years, they are
unable to withstand a supposed intraocular tension produced by
near work. When other errors of refraction, such as
hypermetropia and astigmatism, believed to be congenital, were
present, it has been supposed that the accommodative struggle for
distinct vision produced irritation and strain which encouraged
the production of short sight. When the condition developed in
adults, the explanations had to be modified to fit the case, and the
fact that a considerable number of cases were observed among peasants
and others who did not use their eyes for near work led some
authorities to divide the anomaly into two classes, one caused by
near work and one unrelated to it, the latter being conveniently
attributed to hereditary tendencies.
As
it was impossible to abandon the educational system, attempts
were made to minimize the supposed evil effects of the reading,
writing and other near work which it demanded. Careful and detailed
rules were laid down by various authorities as to the sizes of type
to be used in schoolbooks, the length of the lines, their distance
apart, the distance at which the book should be held, the amount and
arrangement of the light, the construction of the desks, the length
of time the eyes might be used without a change of focus, etc.
Face-rests were even devised to hold the eyes at the prescribed
distance from the desk and to prevent stooping, which was supposed to
cause congestion of the eyeball and thus to encourage elongation. The
Germans, with characteristic thoroughness, actually used these
instruments of torture, Cohn never allowing his own children to
write without one, "even when sitting at the best possible
desk."(2)
The
results of these preventive measures were disappointing. Some
observers reported a slight decrease in the percentage of myopia in
schools in which the prescribed reforms had been made, but on the
whole, as Risley has observed in his discussion of the subject in
Norris and Oliver's System of Diseases of the Eye, "the
injurious results of the educational process were not notably
arrested."
Fig.
56. Face-Rest Designed by Kallmann, a German Optician Cohn
never allowed his children to write without it, even when sitting at
the best possible desk.
"It
is a significant, though discouraging, fact," he continues,
"that the increase, as found by Cohn both in the percentage and
in the degree of myopia, had taken place in those schools where he
had especially exerted himself to secure the introduction of hygienic
reforms; and the same is true of the observations of Just, who had
examined the eyes of twelve hundred and twenty-nine of the pupils of
the two high schools of Zittau, in both of which the hygienic
conditions were all that could be desired. He found, nevertheless,
that the excellent arrangements had not in any degree lessened the
percentage of increase in myopia."(3)
Further
study of the subject has only added to its difficulty, while at the
same time it has tended to relieve the schools of much of the
responsibility formerly attributed to them for the production of
myopia. As the American Encyclopedia of Ophthalmology points out,
"the theory that myopia is due to close work aggravated by town
life and badly lighted rooms is gradually giving ground before
statistics."(4)
In
an investigation in London, for instance, in which the schools were
carefully selected to reveal any differences that might arise from
the various influences, hygienic, social and racial, to which the
children were subjected, the proportion of myopia in the best lighted
building of the group was actually found to be higher than in the one
where the lighting conditions were worst, although the higher degrees
of myopia were more numerous in the latter than in the former. It has
also been found that there is just as much myopia in schools where
little near work is done as in those in which the demand upon the
accommodative power of the eye is greater.(5) It is only a minority
of children, moreover, that become myopic; yet all are subject to
practically the same influences, and even in the same child one eye
may become myopic while the other remains normal. On the theory that
shortsight results from any external influence to which the eye is
exposed it is impossible to account for the fact that under the same
conditions of life the eyes of different individuals and the two eyes
of the same individual behave differently.
Owing
to the difficulty of reconciling these facts on the basis of the
earlier theories, there is now a growing disposition to attribute
myopia to hereditary tendencies;(6) but no satisfactory evidence
on this point has been brought forward, and the fact that primitive
peoples who have always had good eyesight become myopic just as
quickly as any others when subjected to the conditions of civilized
life, like the Indian pupils at Carlisle,(7) seems to be conclusive
evidence against it.
In
spite of the repeated failure of preventive measures based upon
the limitation of near work and the regulation of lighting, desks,
types, etc., the use of the eyes at the nearpoint under unfavorable
conditions is still admitted by most exponents of the heredity
theory as probably, if not certainly, a secondary cause of
myopia. Sidler-Huguenin, however, whose startling conclusions as to
the hopelessness of controlling shortsight were quoted earlier, has
observed so little benefit from such precautions that he believes a
myope may become an engineer just as well as a farmer, or a forester;
and as a result of his experiences with anisometropes, persons
with an inequality of refraction between the two organs of vision, he
even suggests that the use of myopic eyes may possibly be more
favorable to their well-being than their non-use. In 150 cases in
which, owing to this inequality and other conditions, the subjects
practically used but one eye, the weaker organ, he reports,
became gradually more and more myopic, sometimes excessively so, in
open defiance of all the accepted theories relating to the matter.
The
prevalence of myopia, the unsatisfactoriness of all explanations of
its origin, and the futility of all methods of prevention, have led
some writers of repute to the conclusion that the elongated eyeball
is a natural physiological adaptation to the needs of civilization.
Against this view two unanswerable arguments can be brought. One
is that the myopic eye does not see so well even at the near point as
the normal eye, and the other that the defect tends to progression
with very serious results, often ending in blindness. If Nature
has attempted to adapt the eye to civilized conditions by an
elongation of the globe, she has done it in a very clumsy manner. It
is true that many authorities assume the existence of two kinds
of myopia, one physiological, or at least harmless, and the other
pathological; but since it is impossible to say with certainty
whether a given case is going to progress or not, this distinction,
even if it were correct, would be more important theoretically than
practically.
Into
such a slough of despond and contradiction have the misdirected
labors of a hundred years led us ! But in the light of truth the
problem turns out to be a very simple one. In view of the facts given
in Chapters V and IX, it is easy to understand why all previous
attempts to prevent myopia have failed. All these attempts have aimed
at lessening the strain of near work upon the eye, leaving the strain
to see distant objects unaffected, and totally ignoring 4 the mental
strain which underlies the optical one. There are many differences
between the conditions to which the children of primitive man were
subjected, and those under which the offspring of civilized
races spend their developing years, besides the mere fact that the
latter learn things out of books and write things on paper, and the
former did not.
In
the process of education civilized children are shut up for hours
every day within four walls, in the charge of teachers who are too
often nervous and irritable. They. are even compelled to remain for
long periods in the same position. The things they are required to
learn may be presented in such a way as to be excessively
uninteresting; and they are under a continual compulsion to think of
the gaining of marks and prizes rather than the acquisition of
knowledge for its own sake. Some children endure these unnatural
conditions better than others. Many cannot stand the strain, and thus
the schools become the hotbed, not only of myopia, but of all other
errors of refraction.
CITATIONS
1.
A satisfactory explanation of the mechanism by which near work
produces myopia has not yet been given. - Tscherning: Physiologic
Optics, p. 86
It
is not yet determined how near work changes the longitudinal
structure of the eye. - Eversbusch: The Diseases of Children, vol.
vii, p. 291.
2.
The Hygiene of the Eye in Schools, p 127.
3.
School Hygiene, System of Diseases of the Eye, vol. ii, p. 361.
4.
American Encyclopedia and Dictionary of Ophthalmology, edited by
Wood, 1913-1919, vol. xi, p. 8271.
5.
Lawson: Brit. Med. Jour., June 18, 1898.
6.
It seems to have been amply demonstrated, by the studies of Motais,
Steiger, Miss Barrington, and Karl Pearson, that errors of refraction
are inherited. And while the use of the eyes for near work is
probably a secondary cause, determining largely the development of
the defects it is not the primary cause. - Cyclopedia of Education,
edited by Monroe, 1911-1913.
7.
Fox (quoted by Risley): System of Diseases of the Eye, vol. ii, p.
357.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXVII
THE PREVENTION OF MYOPIA AND OTHER ERRORS OF REFRACTION
IN SCHOOLS: A METHOD THAT SUCCEEDED
You
cannot see anything with perfect sight unless you have seen it
before. When the eye looks at an unfamiliar object it always strains
more or less to see that object, and an error of refraction is always
produced. When children look at unfamiliar writing or figures on the
blackboard, distant maps, diagrams or pictures, the retinoscope
always shows that they are myopic, though their vision may be under
other circumstances absolutely normal. The same thing happens when
adults look at unfamiliar distant objects. When the eye regards
a familiar object, however, the effect is quite otherwise. Not
only can it be regarded without strain, but the strain of looking
later at unfamiliar objects is lessened.
This
fact furnishes us with a means of overcoming the mental strain to
which children are subjected by the modern educational system. It is
impossible to see anything perfectly when the mind is under a strain,
and if children become able to relax when looking at familiar
objects, they become able, sometimes in an incredibly brief
space of time, to maintain their relaxation when looking at
unfamiliar objects.
I
discovered this fact while examining the eyes of 1,500 school
children at Grand Forks, N. D., in 1903.1 In many cases children who
could not read all of the letters on the Snellen test card at the
first test read them at the second or third test. After a class had
been examined the children who had failed would sometimes ask for a
second test, and then it often happened that they would read the
whole card with perfect vision. So frequent were these occurrences
that there was no escaping the conclusion that in some way the vision
was improved by reading the Snellen test card. In one class I found a
boy who at first appeared to be very myopic, but who, after a little
encouragement, read all the letters on the test card. The teacher
asked me about this boy's vision, because she had found him to be
very "nearsighted." When I said that his vision was
normal she was incredulous, and suggested that he might have learned
the letters by heart, or been prompted by another pupil. He was
unable to read the writing or figures on the blackboard, she said, or
to see the maps, charts and diagrams on the walls, and did not
recognize people across the street. She asked me to test his sight
again, which I did, very carefully, under her supervision, the
sources of error which she had suggested being eliminated. Again the
boy read all the letters on the card. Then the teacher tested his
sight. She wrote some words and figures on the blackboard, and asked
him to read them. He did so correctly. Then she wrote additional
words and figures, which he read equally well. Finally she asked him
to tell the hour by the clock twenty-five feet distant, which he did
correctly. It was a dramatic situation, both the teacher and the
children being intensely interested. Three other cases in the
class were similar, their vision, which had previously been very
defective for distant objects, becoming normal in the few moments
devoted to testing their eyes. It is not surprising that after such a
demonstration the teacher asked to have a Snellen test card
placed permanently in the room. The children were directed to read
the smallest letters they could see from their seats at least once
every day, with both eyes together and with each eye separately
the other being covered with the palm of the hand in such a way as to
avoid pressure on the eyeball. Those whose vision was defective
were encouraged to read it more frequently, and, in fact, needed
no encouragement to do so after they found that the practice helped
them to see the blackboard, and stopped the headaches, or other
discomfort, previously resulting from the use of their eyes.
In
another class of forty children, between six and eight, thirty of the
pupils gained normal vision while their eyes were being tested. The
remainder were cured later under the supervision of the teacher by
exercises in distant vision with the Snellen card. This teacher had
noted every year for fifteen years that at the opening of the school
in the fall all the children could see the writing on the blackboard
from their seats, but before school closed the following spring
all of them without exception complained that they could not see
it at a distance of more than ten feet. After learning of the
benefits to be derived from the daily practice of distant vision with
familiar objects as the points of fixation, this teacher kept a
Snellen test card continually in her classroom and directed the
children to read it every day. The result was that for eight years no
more of the children under her care acquired defective eyesight.
This
teacher had attributed the invariable deterioration in the
eyesight of her charges during the school year to the fact that her
classroom was in the basement and the light poor. But teachers with
well-lighted classrooms had the same experience, and after the
Snellen test card was introduced into both the well-lighted and the
poorly lighted rooms, and the children read it every day, the
deterioration of their eyesight not only ceased, but the vision of
all improved. Vision which had been below normal improved, in most
cases, to normal, while children who already had normal sight,
usually reckoned at 20/20, became able to read 20/15, or 20/10. And
not only was myopia cured, but the vision for near objects was
improved.
At
the request of the superintendent of the schools of Grand Forks, Mr.
J. Nelson Kelly, the system was introduced into all the schools of
the city and was used continuously for eight years, during which time
it reduced myopia among the children, which I found at the beginning
to be about six per cent, to less than one per cent.
In
1911 and 1912 the same system was introduced into some of the schools
of New York City,1 with an attendance of about ten thousand children.
Many of the teachers neglected to use the cards, being unable to
believe that such a simple method, and one so entirely at variance
with previous teaching on the
subject,
could accomplish the desired results. Others kept the cards in a
closet except when they were needed for the daily eye drill, lest the
children should memorize them. Thus they not only put an unnecessary
burden upon themselves, but did what they could to defeat the purpose
of the system, which is to give the children daily exercise in
distant vision with a familiar object as the point of fixation. A
considerable number, however, used the system intelligently and
persistently, and in less than a year were able to present reports
showing that of three thousand children with imperfect sight over one
thousand had obtained normal vision by its means. Some of these
children, as in the case of the children of Grand Forks, were
cured in a few minutes. Many of the teachers were also cured, some of
them very quickly. In some cases the results of the system were
so astonishing as to be scarcely credible.
In
a class of mental defectives, where the teacher had kept records of
the eyesight of the children for several years, it had been
invariably found that their vision grew steadily worse as the term
advanced. As soon as the Snellen test card had been introduced,
however, they began to improve. Then came a doctor from the Board of
Health who tested the eyes of the children and put glasses on all of
them, even those whose sight was fairly good. The use of the card was
then discontinued, as the teacher did not consider it proper to
interfere while the children were wearing glasses prescribed by a
physician. Very soon, however, the children began to lose,
break, or discard, their glasses. Some said that the spectacles gave
them headaches, or that they felt better without them. In the course
of a month or so most of the aids to vision which the Board of Health
had supplied had disappeared. The teacher then felt herself at
liberty to resume the use of the Snellen test card. Its benefits were
immediate. The eyesight and the mentality of the children
improved simultaneously, and soon they were all drafted into the
regular classes, because it was found that they were making the same
progress in their studies as the other children were.
Another
teacher reported an equally interesting experience. She had a class
of children who did not fit into the other grades. Many of them were
backward in their studies. Some were persistent truants. All of
them had defective eyesight. A Snellen test card was hung in the
classroom where all the children could see it, and the teacher
carried out my instructions literally. At the end of six months all
but two had been cured, and these had improved very much, while the
worst incorrigible and the worst truant had become good students. The
incorrigible, who had previously refused to study, because,
he said it gave him a headache to look at a book, or at the
blackboard, found out that the test card, in some way, did him a lot
of good; and although the teacher had asked him to read it but
once a day, he read it whenever he felt uncomfortable. The
result was that in a few weeks his vision had become normal and his
objection to study had disappeared. The truant had been in the habit
of remaining away from school two or three days every week, and
neither his parents nor the truant officer had been able to do
anything about it. To the great surprise of his teacher he never
missed a day after having begun to read the Snellen test card. When
she asked for an explanation, he told her that what had driven him
away from school was the pain that came in his eyes whenever he tried
to study, or to read the writing on the blackboard. After reading the
Snellen test card, he said, his eyes and head were rested and he was
able to read without any discomfort.
To
remove any doubts that might arise as to the cause of the improvement
noted in the eyesight of the children, comparative tests were made
with and without cards. In one case six pupils with defective sight
were examined daily for one week without the use of the test card. No
improvement took place. The card was then restored to its place, and
the group was instructed to read it every day. At the end of a week
all had improved and five were cured. In the case of another group of
defectives the results were similar. During the week that the card
was not used no improvement was noted; but after a week of exercises
in distant vision with the card all showed marked improvement, and at
the end of a month all were cured. In order that there might be no
question as to the reliability of the records of the teachers some of
the principals asked the Board of Health to send an inspector to test
the vision of the pupils, and whenever this was done the records were
found to be correct.
One
day I visited the city of Rochester, and while there I called on the
Superintendent of Public Schools and told him about my method of
preventing myopia. He was very much interested and invited me to
introduce it in one of his schools. I did so, and at the end of three
months a report was sent to me showing that the vision of all the
children had improved, while quite a number of them had obtained
normal vision in both eyes.
The
method has been used in a number of other cities and always with the
same result. The vision of all the children improved, and many of
them obtained normal vision in the course of a few minutes,
days, weeks, or months.
It
is difficult to prove a negative proposition, but since this system
improved the vision of all the children who used it, it follows
that none could have grown worse. It is therefore obvious that it
must have prevented myopia. This cannot be said of any method of
preventing myopia in schools which had previously been tried. All
other methods are based on the idea that it is the excessive use of
the eyes for near work that causes myopia, and all of them have
admittedly failed.
It
is also obvious that the method must have prevented other
errors of refraction, a problem which previously had not even been
seriously considered, because hypermetropia is supposed to be
congenital, and astigmatism was until recently supposed also to be
congenital in the great majority of cases. Anyone who knows how to
use a retinoscope may, however, demonstrate in a few minutes that
both of these conditions are acquired; for no matter how astigmatic
or hypermetropic an eye may be, its vision always becomes normal when
it looks at a blank surface without trying to see. It may also
be demonstrated that when children are learning to read, write,
draw, sew, or to do anything else that necessitates their
looking at unfamiliar objects at the nearpoint, hypermetropia, or
hypermetropic astigmatism, is always produced. The same is true
of adults. These facts have not been reported before, so far as I am
aware, and they strongly suggest that children need, first of all,
eye education. They must be able to look at strange letters or
objects at the near-point without strain before they can make much
progress in their studies, and in every case in which the method has
been tried it has been proven that this end is attained by daily
exercise in distant vision with the Snellen test card. When their
distant vision has been improved by this means children invariably
become able to use their eyes without strain at the near-point.
The
method succeeded best when the teacher did not wear glasses. In fact,
the effect upon the children of a teacher who wears glasses is
so detrimental that no such person should be allowed to be a
teacher, and since errors of refraction are curable, such a ruling
would work no hardship on anyone. Not only do children imitate the
visual habits of a teacher who wears glasses, but the nervous
strain of which the defective sight is an expression produces in them
a similar condition. In classes of the same grade, with the same
lighting, the sight of children whose teachers did not wear glasses
has always been found to be better than the sight of children whose
teachers did wear them.
In
one case I tested the sight of children whose teacher wore glasses,
and found it very imperfect. The teacher went out of the room on an
errand, and after she had gone I tested them again. The results were
very much better. When the teacher returned she asked about the sight
of a particular boy, a very nervous child, and as I was proceeding to
test him she stood before him and said, "Now, when the doctor
tells you to read the card, do it." The boy couldn't see
anything. Then she went behind him, and the effect was the same as if
she had left the room. The boy read the whole card.
Still
better results would be obtained if we could reorganize the
educational system on a rational basis. Then we might expect a
general return of that primitive acuity of vision which we marvel at
so
greatly
when we read about it in the memoirs of travellers. But even under
existing conditions it has been proven beyond the shadow of a doubt
that errors of refraction are no necessary part of the price we must
pay for education.
There
are at least ten million children in the schools of the United States
who have defective sight. This condition prevents them from taking
full advantage of the educational opportunities which the State
provides. It undermines their health and wastes the taxpayers' money.
If allowed to continue, it will be an expense and a handicap to them
throughout their lives. In many cases it will be a source of
continual misery and suffering. And yet practically all of these
cases could be cured and the development of new ones prevented by the
daily reading of the Snellen test card.
Why
should our children be compelled to suffer and wear glasses for want
of this simple measure of relief ? It costs practically nothing. In
fact, it would not be necessary, in some cases, as in the schools of
New York City, even to purchase the Snellen test cards, as they are
already being used to test the eyes of the children. Not only does it
place practically no additional burden upon the teachers, but,
by improving the eyesight, health, disposition and mentality of
their pupils, it greatly lightens their labors. No one would venture
to suggest, further, that it could possibly do any harm. Why, then,
should there be any delay about introducing it into the schools?
If
there is still thought to be need for further investigation and
discussion, we can investigate and discuss just as well after the
children get the cards as before, and by adopting that course we
shall not run the risk of needlessly condemning another generation
to that curse which heretofore has always dogged the footsteps of
civilization, namely, defective eyesight. I appeal to all who
read these lines to use whatever influence they possess toward the
attainment of this end.
DIRECTIONS
FOR USING THE SNELLEN TEST CARD FOR THE PREVENTION AND CURE OF
IMPERFECT SIGHT IN SCHOOLS
The
Snellen Test Card is placed permanently upon the wall of the
classroom, and every day the children silently read the smallest
letters they can see from their seats with each eye separately, the
other being covered with the palm of the hand in such a way as to
avoid pressure on the eyeball. This takes no appreciable amount of
time, and is sufficient to improve the sight of all children in
one week and to cure all errors of refraction after some months, a
year, or longer.
Children
with markedly defective vision should be encouraged to read the card
more frequently. Children wearing glasses should not be
interfered with, as they are supposed to be under the care of a
physician, and the practice will do them little or no good while
the glasses are worn.
While
not essential, it is a great advantage to have records made of the
vision of each pupil at the time when the method is introduced, and
thereafter at convenient intervals - annually or more frequently.
This may be done by the teacher. The records should include the name
and age of the pupils, the vision of each eye tested at twenty feet,
and the date. For example:
John
Smith, 10, Sept. 15, 1919
R. V. (vision of
the right eye) 20/40
L. V. (vision of the
left eye) 20/20
John Smith, 11, January 1, 1920
R.
V. 20/30
L. V. 20/15
A
certain amount of supervision is absolutely necessary. At least
once a year some one who understands the method should visit each
classroom for the purpose of answering questions, encouraging
the teachers to continue the use of the method, and making some
kind of a report to the proper authorities. It is not necessary that
either the supervisor, the teachers. or the children, should
understand anything about the physiology of the eye.
CITATIONS
1.
Bates: The Prevention of Myopia in School Children, N. Y. Med.
Jour., July 29, 1911.
2.
Bates: Myopia Prevention by Teachers, N. Y. Med. Jour., Aug. 30,
1913.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXVIII
THE STORY OF EMILY
The
efficacy of the method of treating imperfect sight without glasses
presented in this book has been demonstrated in thousands of cases,
not only in my own practice but in that of many persons of whom I may
not even have heard; for almost all patients, when they are
cured, proceed to cure others. At a social gathering one evening, a
lady told me that she had met a number of my patients; but when she
mentioned their names, 1 found that I did not remember any of them
and said so.
"That
is because you cured them by proxy," she said. "You didn't
directly cure Mrs. Jones or Mrs. Brown, but you cured Mrs. Smith, and
Mrs. Smith cured the other ladies. You didn't treat Mr. and Mrs.
Simpkins, or Mr. Simpkins' mother and brother; but you may remember
that you cured Mr. Simpkins' boy of a squint, and he cured the rest
of the family."
In
schools where the Snellen test card was used to prevent and cure
imperfect sight, the children, after they were cured themselves,
often took to the practice of ophthalmology with the greatest
enthusiasm and success, curing their fellow students, their
parents and their friends. They made a kind of game of the treatment,
and the progress of each school case was watched with the most
intense interest by all the children. On a bright day, when the
patients saw well, there was great rejoicing, and on a dark day there
was corresponding depression. One girl cured twenty-six children in
six months; another cured twelve in three months; a third developed
quite a varied ophthalmological practice, and did things of which
older and more experienced practitioners might well have been proud.
Going to the school which she attended one day, I asked this girl
about her sight, which had been very imperfect. She replied that it
was now very good, and that her headaches were quite gone. I tested
her sight and found it normal. Then another child whose sight had
also been very poor spoke up.
"I
can see all right too," she said. "Emily" -
indicating girl No. l - "cured me."
"Indeed!"
I replied. "How did she do that?"
The
second girl explained that Emily had had her read the card, which she
could not see at all from the back of the room, at a distance of a
few feet. The next day she had moved it a little farther away, and so
on, until the patient was able to read it from the back of the room,
just as the other children did. Emily now told her to cover the right
eye and read the card with her left, and both girls were
considerably upset to find that the uncovered eye was
apparently blind. The school doctor was consulted and said that
nothing could be done. The eye had been blind from birth and no
treatment would do any good.
Nothing
daunted, however, Emily undertook the treatment. She told the patient
to cover her good eye and go up close to the card, and at a distance
of a foot or less it was found that she could read even the small
letters. The little practitioner then proceeded confidently as
with the other eye, and after many months of practice the patient
became the happy possessor of normal vision in both eyes. The case
had, in fact, been simply one of high myopia, and the school doctor,
not being a specialist, had not detected the difference between this
condition and blindness.
In
the same classroom, there had been a little girl with congenital
cataract, but on the occasion of my visit the defect had disappeared.
This, too, it appeared, was Emily's doing. The school doctor had said
that there was no help for this eye except through operation, and as
the sight of the other eye was pretty good, he fortunately did not
think it necessary to urge such a course. Emily accordingly took the
matter in hand. She had the patient stand close to the card, where,
with the good eye covered, she was unable to see even the big C.
Emily now held the card between the patient and the light, and moved
it back and forth. At a distance of three or four feet this movement
could be observed indistinctly by the patient. The card was then
moved farther away, until the patient became able to see it move at
ten feet and to see some of the larger letters indistinctly at a less
distance. Finally; after six months, she became able to read the card
with the bad eye as well as with the good one. After testing her
sight and finding it normal in both eyes, I said to Emily:
"You
are a splendid doctor. You beat them all. Have you done anything
else?"
The
child blushed, and turning to another of her classmates, said:
"Mamie,
come here."
Mamie
stepped forward and I looked at her eyes. There appeared to be
nothing wrong with them.
"I
cured her," said Emily.
"What
of ?" I inquired.
"Cross
eyes," replied Emily.
"How?"
I asked, with growing astonishment.
Emily
described a procedure very similar to that adopted in the other
cases. Finding that the sight of the crossed eye was very poor, so
much so, indeed, that poor Mamie could see practically nothing with
it, the obvious course of action seemed to her to be the restoration
of its sight; and, never having read any medical literature, she did
not know that this was impossible. So she went to it. She had Mamie
cover her good eye and practice the bad one at home and at school,
until at last the sight became normal and the eye straight. The
school doctor had wanted to have the eye operated upon, I was told,
but, fortunately, Mamie was "scared" and would not consent.
And here she was with two perfectly good, straight eyes.
"Anything
else?" I inquired, when Mamie's case had been disposed of. Emily
blushed again, and said:
"Here's
Rose. Her eyes used to hurt her all the time, and she couldn't see
anything on the blackboard. Her headaches used to be so bad that
she had to stay away from school every once in a while. The doctor
gave her glasses; but they didn't help her, and she wouldn't wear
them. When you told us the card would help our eyes I got busy with
her. I had her read the card close up, and then I moved it farther
away, and now she can see all right, and her head doesn't ache any
more. She comes to school every day, and we all thank you very much."
This
was a case of compound hypermetropic astigmatism.
Such
stories might be multiplied indefinitely. Emily's astonishing record
cannot, it is true, be duplicated; but lesser cures by cured patients
have been very numerous, and serve to show that the benefits of the
method of preventing and curing defects of vision in the schools
which is presented in the foregoing chapter would be far-reaching.
Not only errors of refraction would be cured, but many more serious
defects; and not only the children would be helped, but their
families and friends also.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXIX
MIND AND VISION
Poor
sight is admitted to be one of the most fruitful causes of
retardation in the schools. It is estimated(1) that it may
reasonably be held responsible for a quarter of the habitually
"left-backs," and it is commonly assumed that all this
might be prevented by suitable glasses.
There
is much more involved in defective vision, however, than mere
inability to see the blackboard, or to use the eyes without pain or
discomfort. Defective vision is the result of an abnormal condition
of the mind; and when the mind is in an abnormal condition it is
obvious that none of the processes of education can be conducted with
advantage. By putting glasses upon a child we may, in some
cases, neutralize the effect of this condition upon the eyes, and by
making the patient more comfortable may improve his mental
faculties to some extent; but we do not alter fundamentally the
condition of the mind, and by confirming it in a bad habit we
may make it worse.
It
can easily be demonstrated that among the faculties of the mind
which are impaired when the vision is impaired is the memory; and as
a large part of the educational process consists of storing the mind
with facts, and all the other mental processes depend upon one's
knowledge of facts, it is easy to see how little is accomplished by
merely putting glasses on a child that has "trouble with its
eyes." The extraordinary memory of primitive people
has been attributed to the fact that owing to the absence of any
convenient means of making written records they had to depend upon
their memories, which were strengthened accordingly; but in view of
the known facts about the relation of memory to eyesight it is more
reasonable to suppose that the retentive mem
ory
of primitive man was due to the same cause as his keen vision,
namely, a mind at rest.
The
primitive memory as well as primitive keenness of vision, has been
found among civilized people; and if the necessary tests had been
made it would doubtless have been found that they always occur
together, as they did in a case which recently came under my
observation. The subject was a child of ten with such marvelous
eyesight that she could see the moons of Jupiter with the naked eye,
a fact which was demonstrated by her drawing a diagram of these
satellites which exactly corresponded to the diagrams made by persons
who had used a telescope. Her memory was equally remarkable. She
could recite the whole content of a book after reading it, as Lord
Macaulay is said to have done, and she learned more Latin in a few
days without a teacher than her sister, who had six diopters of
myopia, had been able to do in several years. She remembered five
years afterward what she ate at a restaurant, she recalled the name
of the waiter, the number of the building and the street in which it
stood. She also remembered what she wore on this occasion and what
every one else in the party wore. The same was true of every other
event which had awakened her interest in any way, and it was a
favorite amusement in her family to ask her what the menu had been
and what people had worn on particular occasions.
When
the sight of two persons is different, it has been found that their
memories differ in exactly the same degree. Two sisters, one of whom
had only ordinary good vision, indicated by the formula 20/20, while
the other had 20/10, found that the time it took them to learn eight
verses of a poem varied in almost exactly the same ratio as their
sight. The one whose vision was 20/10 learned eight verses of the
poem in fifteen minutes, while the one whose vision was only 20/20
required thirty-one minutes to do the same thing. After palming, the
one with ordinary vision learned eight more verses in twenty-one
minutes, while the one with 20/10 was able to reduce her time by only
two minutes, a variation clearly within the limits of error. In other
words,
the mind of the latter being already in a normal or nearly normal
condition, she could not improve it appreciably by palming, while the
former, whose mind was under a strain, was able to gain relaxation,
and hence improve her memory, by this means.
Even
when the difference in sight is between the two eyes of the same
person it can be demonstrated, as was pointed out in the
chapter on "Memory as an Aid to Vision," that there is a
corresponding difference in the memory, according to whether both
eyes are open, or the better eye closed.
Under
the present educational system there is a constant effort to compel
the children to remember. These efforts always fail. They spoil
both the memory and the sight. The memory cannot be forced any more
than the vision can be forced. We remember without effort, just
as we see without effort, and the harder we try to remember or see
the less we are able to do so.
The
sort of things we remember are the things that interest us, and the
reason children have difficulty in learning their lessons is because
they are bored by them. For the same reason, among others, their
eyesight becomes impaired, boredom being a condition of mental
strain in which it is impossible for the eye to function normally.
Some
of the various kinds of compulsion now employed in the
educational process may have the effect of awakening interest. Betty
Smith's interest in winning a prize, for instance, or in merely
getting ahead of Johnny Jones, may have the effect of rousing
her interest in lessons that have hitherto bored her, and this
interest may develop into a genuine interest in the acquisition
of knowledge; but this cannot be said of the various fear incentives
still so largely employed by teachers. These, on the contrary, have
the effect, usually, of completely paralyzing minds already benumbed
by lack of interest, and the effect upon the vision is equally
disastrous.
The
fundamental reason, both for poor memory and
poor
eyesight in school children, in short, is our irrational and
unnatural educational system.
Montessori
has taught us that it is only when children are interested that
they can learn. It is equally true that it is only when they are
interested that they can see. This fact was strikingly illustrated in
the case of one of the two pairs of sisters mentioned above.
Phebe, of the keen eyes, who could recite whole books if she happened
to be interested in them, disliked mathematics and anatomy
extremely, and not only could not learn them but became myopic
when they were presented to her mind. She could read letters a
quarter of an inch high at twenty feet in a poor light, but when
asked to read figures one to two inches high in a good light at ten
feet she miscalled half of them. When asked to tell how much 2 and 3
made, she said "4," before finally deciding on "5":
and all the time she was occupied with this disagreeable subject
the retinoscope showed that she was myopic. When I asked her to
look into my eye with the ophthalmoscope, she could see nothing,
although a much lower degree of visual acuity is required to note the
details of the interior of the eye than to see the moons of Jupiter.
Shortsighted
Isabel, on the contrary, had a passion for mathematics and anatomy,
and excelled in those subjects. She learned to use the ophthalmoscope
as easily as Phebe had learned Latin. Almost immediately she saw
the optic nerve, and noted that the center was whiter than the
periphery. She saw the light-colored lines, the arteries; and the
darker ones, the veins; and she saw the light streaks on the
blood-vessels. Some specialists never become able to do this, and no
one could do it without normal vision. Isabel's vision, therefore,
must have been temporarily normal when she did it. Her vision for
figures, although not normal, was better than for letters.
In
both these cases the ability to learn and the ability to see went
hand in hand with interest. Phebe could read a photographic reduction
of the Bible and recite what she had read verbatim, she could see
the
moons of Jupiter and draw a diagram of them afterwards, because she
was interested in these things; but she could not see the interior of
the eye, nor see figures even half as well as she saw letters,
because these things bored her. When, however, it was suggested to
her that it would be a good joke to surprise her teachers, who were
always reproaching her for her backwardness in mathematics, by taking
a high mark in a coming examination, her interest in the subject
awakened and she contrived to learn enough to get seventy-eight per
cent. In Isabel's case letters were antagonistic. She was not
interested in most of the subjects with which they dealt, and,
therefore, she was backward in those subjects, and had become
habitually myopic. But when asked to look at objects which aroused an
intense interest her vision became normal.
When
one is not interested, in short, one's mind is not under control, and
without mental control one can neither learn nor see. Not only the
memory but all other mental faculties are improved when the eyesight
becomes normal. It is a common experience with patients cured of
defective sight to find that their ability to do their work has
improved.
The
teacher whose letter is quoted in a later chapter testified that
after gaining perfect eyesight she "knew better how to get at
the minds of the pupils," was "more direct, more definite,
less diffused, less vague," possessed, in fact, "central
fixation of the mind." In another letter she said: "The
better my eyesight becomes the greater is my ambition. On the days
when my sight is best I have the greatest anxiety to do things."
Another
teacher reported that one of her pupils used to sit doing nothing all
day long, and apparently was not interested in anything. After the
test card was introduced into the classroom and his sight improved,
he became anxious to learn, and speedily developed into one of the
best students in the class. In other words his eyes and his mind
became normal together.
A
bookkeeper nearly seventy years of age who had worn glasses for forty
years found after he had
gained
perfect sight without glasses that he could work more rapidly and
accurately and with less fatigue than ever in his life before. During
busy seasons, or when short of help, he has worked for some weeks at
a time from 7 a. m. until 11 p. m., and he insisted that he felt less
tired at night after he was through than he did in the morning when
he started. Previously, although he had done more work than any other
man in the office, it always tired him very much.
He
also noticed an improvement in his temper. Having been so long
in the office, and knowing so much more about the business than his
fellow employees, he was frequently appealed to for advice.
These interruptions, before his sight became normal, were very
annoying to him, and often caused him to lose his temper. Afterward,
however, they caused him no irritation whatever.
In
another case, symptoms of insanity were relieved when the vision
became normal. The patient was a physician who had been seen by many
nerve and eye specialists before he came to me, and who consulted me
at last, not because he had any faith in my methods, but because
nothing else seemed to be left for him to do. He brought with him
quite a collection of glasses prescribed by different men, no two of
them being alike. He had worn glasses, he told me, for many months at
a time without benefit, and then he had left them off and had been
apparently no worse.
Outdoor
life had also failed to help him. On the advice of some prominent
neurologists he had even given up his practice for a couple of years
to spend the time upon a ranch, but the vacation had done him no
good.
I
examined his eyes and found no organic defects and no error of
refraction. Yet his vision with each eye was only three-fourths of
the normal, and he suffered from double vision and all sorts of
unpleasant symptoms. He used to see people standing on their
heads, and little devils dancing on the tops of the high buildings.
He also had other illusions too numerous to be mentioned here. At
night his sight was so bad that he had difficulty in finding his way
about, and when walking along a country road he believed that he saw
better when he turned his eyes far to one side and viewed the road
with the side of the retina instead of with the center. At variable
intervals, without warning and without loss of consciousness, he had
attacks of blindness. These caused him great uneasiness, for he was a
surgeon with a large and lucrative practice, and he feared that he
might have an attack while operating.
His
memory was very poor. He could not remember the color of the eyes of
any member of his family, although he had seen them all daily for
years. Neither could he recall the color of his house, the
number of rooms on the different floors, or other details. The faces
and names of patients and friends he recalled with difficulty, or not
at all.
His
treatment proved to be very difficult, chiefly because he had an
infinite number of erroneous ideas about physiological optics in
general and his own case in particular, and insisted that all these
should be discussed; while these discussions were going on he
received no benefit. Every day for hours at a time over a long period
he talked and argued. His logic was wonderful, apparently
unanswerable, and yet utterly wrong.
His
eccentric fixation was of such high degree that when he looked at a
point forty-five degrees to one side from of the big C on the Snellen
test card, he saw the letter just as black as when he looked directly
at it. The strain to do this was terrific, and produced much
astigmatism; but the patient was unconscious of it, and could not be
convinced that there was anything abnormal in the symptom. If he saw
the letter at all, he argued, he must see it as black as it really
was, because he was not color-blind. Finally he became able to look
away from one of the smaller letters on the card and see it worse
than when he looked directly at it. It took eight or nine months to
accomplish this, but when it had been done the patient said that it
seemed as if a great burden had been lifted from his mind. He
experienced a wonderful feeling of rest and relaxation
throughout his whole body.
When
asked to remember black with his eyes closed and covered he said he
could not do so, and he saw every color but the black which one ought
normally to see when the optic nerve is not subject to the stimulus
of light. He had, however, been an enthusiastic football player
at college, and he found at last that he could remember a black
football. I asked him to imagine that this football had been thrown
into the sea and that it was being carried outward by the tide,
becoming constantly smaller but no less black. This he was able to
do, and the strain floated with the football, until, by the time the
latter had been reduced to the size of a period in a newspaper, it
was entirely gone.
The
relief continued as long as he remembered the black spot, but as he
could not remember it all the time, I suggested another method of
gaining permanent relief. This was to make his sight
voluntarily worse, a plan against which he protested with
considerable emphasis. "Good heavens!" he said. "Isn't
my sight bad enough without making it worse ?"
After
a week of argument, however, he consented to try the method, and the
result was extremely satisfactory. After he had learned to see
two or more lights where there was only one, by straining to see a
point above the light while still trying to see the light as well as
when looking directly at it, he became able to avoid the
unconscious strain that had produced his double and multiple vision
and was not troubled by these superfluous images any more. In a
similar manner other illusions were prevented.
One
of the last illusions to disappear was his belief that an effort was
required to remember black. His logic on this point was overwhelming,
but after many demonstrations he was convinced that no effort was
required to let go; and when he realized this, both his vision and
his mental condition immediately improved.
He
finally became able to read 20/10 or more, and although more than
fifty-five years of age, he also read diamond type at from six to
twenty-four inches. His night blindness was relieved, his
attacks of day blindness ceased, and he told me the color of the eyes
of his wife and children. One day he said to me: "Doctor, I
thank you for what you have done for
my
sight; but no words can express the gratitude I feel for what you
have done for my mind." Some years later he called with his
heart full of gratitude, because there had been no relapse.
From
all these facts it will be seen that the problems of vision are
far more intimately associated with the problems of education than we
had supposed, and that they can by no means be solved by putting
concave, or convex, or astigmatic lenses before the eyes of the
children.
CITATIONS
1.
School Health News, published by the Department of Health of Near
York City, February, 1919.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXX
NORMAL SIGHT AND THE RELIEF OF PAIN FOR SOLDIERS AND
SAILORS
The
Great War is over, and among the millions of brave men who laid down
their lives in the cruel conflict there were some who thought
that they were doing so that wars might be no more. But the earth IS
still filled with wars and rumors of war, and in the countries of the
victorious Allies the spirit of militarism is rampant. In the United
States we are being urged to increased naval and military
expenditure, and there is a strong demand for universal military
training. Whether it is necessary for us to join in the competition
of armaments which resulted in the terrific convulsion through which
we have just passed, is a question which need not be entered into
here; but if we are going to do so, we may as well have soldiers and
sailors with normal sight; and if we attain this end we shall not
have borne the burdens of militarism and navalism altogether in vain.
After
the United States entered the recent war, I had the privilege of
making it possible for many young men who had been unable to meet the
visual requirements for admission to the army and navy, or to
favorite branches of these services, to gain normal vision; and
seeing no reason why such benefits should be confined to the
few, I supplied the Surgeon General of the Army with a plan
whereby with far less trouble and expense than was involved by the
optical service upon which we were then depending to make the
worst of the enlisted eye-defectives available for service at
the front, normal vision without glasses might have been insured to
all soldiers and sailors. This plan was not acted upon, and I
now present it, with some modifications, to the public, in the
hope that enough people will see its military value to secure
its adoption.
If
we are to have universal military training, we shall find, as the
nations of Europe have found, that it will be necessary to take
measures to provide suitable material for such training. In
Europe this necessity has resulted in extensive systems of
child care, but in this book we are concerned only with the question
of eyesight. In the first draft for the recent war, defective
eyesight was the greatest single cause for rejection, while in later
drafts it became one of three leading causes only because of an
enormous lowering of an already low standard.
Yet
there is no impediment to the raising of an army which might be more
easily removed. If we want our children to grow big enough to be
soldiers, without losing most of their teeth and developing flat feet
and crooked spines before they reach the military age, we shall have
to make some arrangements, as every one of the advanced countries of
Europe has done, for providing material as well as intellectual food
in the schools. We shall have to employ school physicians on full
time, and pay them enough to compensate men of eminence for the
loss of private practice. We shall also have to see that the
children are not sacrificed to the ignorance or poverty of their
parents before they reach school age. But to preserve their eyesight
it is only necessary to place Snellen test cards in every school
classroom, and see that the children read them every day. With this
simple system of eye education beginning in the kindergarten and
extending through the whole educational process up to the
university and the professional school, it would soon be found
that the young men of the country, on arrival at the military age,
were practically free from eye defects.
But
some years must elapse before this happy result can be achieved; and
all eyes, moreover, no matter how good their vision, are benefited by
the daily practice of the art of seeing, while by such practice those
visual lapses to which every eye is subject, and which are
particularly dangerous in military and naval operations, are either
prevented or minimized. Therefore a system of eye education for
training camps and the front should also be provided. For this
purpose the method used in the schools could be modified.
Under
conditions of actual warfare, or on the parade grounds of training
camps, a Snellen test card might be impracticable; but there are
other letters, or small objects,. On the uniforms, on the guns, on
the wagons, or elsewhere, which would serve the purpose equally well.
Letters
or objects which require a vision of 20/20 should be selected by some
one who has been taught what 20/20 means, and the men should be
required to regard these letters or objects twice a day. After
reading the letters they should be directed to cover their closed
eyes with the palms of their hands to shut out all the light, and
remember some color, preferably black, as well as they are able to
see it, for half a minute. Then they should read the letters again
and note any improvement in vision. The whole procedure would take
not more than a minute. It should be made part of the regular drill,
night and morning, and men with imperfect sight should be encouraged
to repeat it as many times a day as convenient. They will need no
urging; for imperfect vision is a bar to advancement, and excludes
from the favorite branch of the service, namely, aviation.
In
each regiment every ten men should be under the supervision of one
man who understands the method, and who must possess normal vision
without glasses. He should carry a pocket test card, consisting of a
few of the smaller letters, and should test the vision of the men at
the beginning of the training, and thereafter at intervals of three
months, reporting the results to the medical officer in charge.
Since
errors of refraction are curable, no soldier should be allowed to
wear glasses; but if the use of these aids to vision is permitted,
the men wearing them should not be required to take part in the eye
drills. as the method will do them no good under these conditions.
When they see the benefits of eye education, however, they may wish
to share them, and will, no doubt, be willing to submit to the
inconvenience resulting, temporarily, from going without their
glasses.
In
military colleges the same method could be used as in the schools;
but a daily eye drill should also form part of the maneuvers on the
parade ground, so that the students may be prepared to use it later
in training camps, or at the front.
To
aviators, whether engaged in military or civilian operations, or
whether they are flying merely for pleasure, eye education is of
particular importance. Accidents to aviators, otherwise
unaccountable, are easily explained when one understands how
dependent the aviator is upon his eyesight, and how easily
perfect vision may be lost amid the unaccustomed surroundings, the
dangers and hardships of the upper air. It was formerly supposed
that aviators maintained their equilibrium in the air by the aid of
the internal ear; but it is now becoming evident from the testimony
of aviators who have found themselves emerging from a cloud with
one wing down, or even with their machines turned completely upside
down, that equilibrium is maintained almost entirely, if not
altogether, by the sense of sight.(1) If the aviator loses his sight,
therefore, he is lost, and we have one of those "unaccountable"
accidents which, during the war, were so unhappily common in the air
service. All aviators, therefore, should make a daily practice of
reading small, familiar letters, or observing other small,
familiar objects, at a distance of ten feet or more. In addition,
they should have a few small letters, or a single letter, on their
machines, at a distance of five, ten, or more feet from their
eyes, arrangements being made to illuminate them for night flying and
fogs, and should read them frequently while in the air. This would
greatly lessen the danger of visual lapses, with their accompanying
loss of equilibrium and judgment.
As
has already been pointed out, eye education not only improves the
sight, but affords a means by which pain, fatigue, the symptoms of
disease and other discomforts, can be relieved. For this latter
purpose it is of the greatest value to solders and sailors; and if,
during the recent war, they had only understood the simple and always
available method of relieving pain by the aid of the memory, not only
much suffering, but many deaths from the destructive effects of
pain upon the body, might have been prevented. A soldier in a flooded
trench, if he can remember black perfectly, will know the
temperature of the water, but will not suffer from cold. Under
the same conditions he may succumb from weakness on the march, but
will not feel fatigue. He may die of hemorrhage, but he will die
painlessly. It will not be necessary to give him morphine to relieve
his pain; and thus to the dangers of the battlefields will not be
added the danger of returning to civil life under the handicap of a
lifelong morphine habit.
This
danger, there is reason to believe, assumed enormous proportions
during the war. The Germans-used a bullet which broke when it struck
the bone and caused intense pain. The men often died of this pain
before help arrived. When they were rescued the surgeons at once gave
them morphine. A few hours later the injection was probably repeated.
Then the drug was given less frequently, but in many cases it was not
discontinued entirely while the man was in the hospital. A Red Cross
surgeon at a meeting of the New York County Medical Society
stated that he had been responsible for producing the morphine
habit in thousands of soldiers, and that every physician at the front
had done the same. By such a simple method as palming all this might
have been prevented.
If
we are going to have universal military and naval training, an
essential part of that training should be the instruction of the
prospective soldiers and sailors in the art of relieving their
own pain; and in the event of war every one who goes to the front, in
whatever capacity, from the generals and admirals down to the
ambulance drivers, should understand palming. Everyone in the war
zone, no matter how far behind the lines, may need this knowledge to
relieve his own pain, and everyone may need it to relieve the pain of
others.
CITATIONS
1.
Anderson: Lancet, March 16, 1918, p. 398; Hucks; Scientific American,
October 6, 1917, p. 263.
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXXI
LETTERS FROM PATIENTS
The
following letters have been selected almost at random from the
author's mail-bag, and are only specimens of many more that are
equally interesting. They are published: because it was s felt that
the personal stories of patients, told in their own language,
might be more interesting and helpful to many readers than the more
formal presentation of the facts in the preceding chapters.
ARMY
OFFICER CURES HIMSELF
AS
noted in the chapter on What Glasses Do to Us, the sight always
improves when glasses are discarded, though this improvement may
be so slight as not to be noticed. In a few unusual cases the
patients, when freed from the handicap of a condition which
compels them to keep their eyes continually under a strain, find out,
in some way, how to avoid strain, and thus regain a greater or less
degree of their normal visual power. The writer of the following
letter was able, without any help from anyone, to discover and put
into practice the main principles presented i 1 this book, and thus
became able to read without his glasses. He is an engineer, and at
the time the letter was written was fifty-one years of age. He had
worn glasses since 1896, first for astigmatism, getting stronger ones
every couple of years, and then for astigmatism and presbyopia. At
one time he asked his oculist and several opticians if the eyes could
not be strengthened by exercises, so as to make glasses unnecessary,
but they said: "No. Once started on glasses you must keep to
them." When the war broke out he was very nearly disqualified
for service in the Expeditionary Forces by his eyes, but managed to
pass the required tests, after which he was ordered abroad as an
officer in the Gas Service. While there he saw in the Literary Digest
of May 2, 1918, a reference to my method of curing defective eyesight
without glasses, and on
May
11 he wrote to me in part as follows:
"At
the front I found glasses a horrible nuisance, and they could not be
worn with gas masks. After I had been about six months abroad I asked
an officer of the Medical Corps about going without glasses.
He said I was right in my ideas and told me to try it. The first week
was awful, but I persisted and only wore glasses for reading and
writing. I stopped smoking at the same time to make it easier on my
nerves.
"I
brought to France two pairs of bow spectacles and two extra lenses
for repairs. I have just removed the extra piece for near vision
from these extra lenses and had them mounted as pince-nez, with
shur-on mounts, to use for reading and writing, so that the only
glasses I now use are for astigmatism, the age lens being off.
Three months ago I could not read ordinary head-line type in
newspapers without glasses. To-day, with a good light, I can read
ordinary book type, held at a distance of eighteen inches from my
eyes. Since the first week in February, when I discarded my
glasses, I have had no headaches, stomach trouble, or dizziness, and
am in good health generally. My eyes are coming back, and I believe
it is due to sticking it out. I ride considerably in automobiles
and trams, and somehow the idea has crept into my mind that after
every trip my eyes are stronger. This, I think, is due to the rapid
changing of focus in viewing scenery going by so fast. Other men
have tried this plan on my advice, but gave it up after two or three
days. Yet, from what they say, I believe they were not so
uncomfortable as I was for a week or ten days. I believe most
people wear glasses because they 'coddle' their eyes."
The
patient was right in thinking that the motor and tram rides improved
his sight. The rapid motion compelled rapid shifting.
A
TEACHER'S EXPERIENCES
It
has frequently been pointed out in this book that imperfect vision is
always associated with an abnormal state of the mind, and that
when the vision improves the mental faculties improve also, to a
greater or less degree. The following letter is a striking
illustration of this fact. The writer, a teacher forty years of age,
was first treated on March 28, 1919. She was wearing the following
glasses: right eye, convex 0.75D.S. with convex 4.00D.C., 105 deg.;
left eye, convex 0.75D.S. with convex 3.50D.C., 105 deg. On June 9,
1919, she wrote:
"I
will tell you about my eyes, but first let me tell you other things.
You were the first to unfold your theories to me, and I found them
good immediately - that is, I was favorably impressed from the start.
I did not take up the cure because other people recommended
it, but because I was convinced: first, that you believed in your
discovery yourself; second, that your theory of the cause of eye
trouble was true. I don't know how I knew these two things, but I
did. After a little conversation with you, you and your discovery
both seemed to me to bear the ear-marks of the genuine article. As to
the success of the method with myself I had a little doubt. You might
cure others, but you might not be able to cure me. However, I took
the plunge, and it has made a great change in me and my life.
"To
begin with, I enjoy my sight. I love to look at things, to examine
them in a leisurely, thorough way, much as a child examines things. I
never realized it at the time, but it was irksome for me to look at
things when I was wearing glasses, and I did as little of it as
possible. The other day, going down on the Sandy Hook boat, I enjoyed
a most wonderful sky without that hateful barrier of misted glasses,
- and I am positive I distinguished delicate shades of color that I
never would have been able to see, even with clear glasses. Things
seem to me now to have more form, more reality, than when I wore
glasses. Looking into the mirror you see a solid representation
on a flat surface, and the flat glass can't show you anything really
solid. My eyeglasses, of course, never gave me this impression, but
one curiously like it. I can see so clearly without them that it is
like looking around corners without changing the position. I
feel that I can almost do it.
"I
very seldom have occasion to palm. Once in a great while I feel the
necessity of it. The same with remembering a period. Nothing else is
ever necessary. I seldom think of my eyes, but at times it is
borne in upon me how much I do use and enjoy using them.
"My
nerves are much better. I am more equable, have more poise, I am less
shy. I never used to show that I was shy, or lacked confidence. I
used to go ahead and what was required, if not without hesitation;
but it was hard. Now I find it easy. Glasses, or poor sight rather,
made me self-conscious. It certainly is a great defect, and one
people are sensitive to without realizing it. I mean the poor sight
and the necessity for wearing glasses. I put on a pair of glasses
the other day just for an experiment, and I found that they magnified
things. My skin looked as if under a magnifying glass. Things seemed
too near. The articles on my chiffonier looked so close I felt like
pushing them away from me. The glasses I especially wanted to
push away. They brought irritation at once. I took them off and felt
peaceful. Things looked normal.
"From
the beginning of the treatment I could use my eyes pretty well, but
they used to tire. I remember making a large Liberty Loan poster
two weeks after I took off my glasses, and I was amazed to find I
could make the whole layout almost perfectly without a ruler just as
well as with my glasses. When I came to true it up with the ruler I
found only the last row of letters a bit out of line at the very end.
I couldn't have done better with glasses. However this wasn't fine
work. About the same time I sewed a hem at night in a black dress,
using a fine needle. I suffered a little for this but not much. I
used to practice my exercises at that time, and palm faithfully.
Now I don't have to practice, or palm; I feel no discomfort, and I am
absolutely unsparing in my use of my eyes. I do everything I want to
with them. I shirk nothing, pass up no opportunity of using them.
From the first I did all my school work, read every notice, wrote all
that was necessary, neglected nothing.
"Now
to sum up the school end of it: I used to get headaches at the end of
the month from adding columns of figures necessary to reports, etc.
Now I do not get them. I used to get flustered when people came into
my room. Now I do not; I welcome them. It is a pleasant change to
feel this way. And - I suppose this is most important really, though
I think of it last - I teach better. I know how to get at the mind
and how to make the children see things in perspective. I gave a
lesson on the horizontal cylinder recently, which, you know, is
not a thrillingly interesting subject, and it was a remarkable lesson
in its results and in the grip it got on every girl in the room,
stupid or bright. What you have taught me makes me use the memory and
imagination more, especially the latter, in teaching.
"To
sum up the effect of being cured upon my own mind: I am more direct,
more definite, less diffused, less vague. In short, I am conscious of
being better centered. It is central fixation of the mind. I saw this
in your latest paper, but I realized it long ago and knew what to
call it."
A
MENTAL TRANSITION
A
man of forty-four who had worn glasses since the age of twenty was
first seen on October 8, 1917, when he was suffering, not only from
very imperfect sight, but from headache and discomfort. He was
wearing for the right eye concave 5.00D.S. with concave 0.50D.C., 180
degrees, and for the left concave 2.50D.S. with concave 1.50D.C., 180
degrees. As his visits were not very frequent and he often went back
to his glasses, his progress was slow. But his pain and discomfort
were relieved very quickly, and almost from the beginning he had
flashes of greatly improved and even of normal vision. This
encouraged him to continue, and his progress, though slow, was
steady. He has now gone without his glasses entirely for some months,
and his nervous condition has improved as much as his sight. His
wife was particularly impressed with the latter effect, and in
December, 1919, she wrote:
"I
have become very much interested in the thought of renewing my youth
by becoming like a little child. The idea of the mental transition is
not unfamiliar, but that this mental, or I should say spiritual,
transition should produce a physical effect, which would lead to
seeing clearly, is a sort of miracle very possible indeed, I should
suppose, to those who have faith.
"In
my husband's case, certainly, some such miracle was wrought; for not
only was he able to lay aside his spectacles after many years
constant use, and to see to read in almost any light, but I
particularly noticed his serenity of mind after treatments. In this
serenity he seemed able to do a great deal of work efficiently, and
not under the high nervous pressure whose after-effect is the
devastating scattering of forces.
"It
did not occur to me for a long time that perhaps your treatment w as
quieting his nerves. But I think now that the quiet periods of
relaxation, two or three times a day, during which he practiced with
the letter card, must have had a very beneficial effect. He is so
enthusiastic by nature, and his nerves are so easily stimulated, that
for years he used to overdo periodically. Of course, his greatly
improved eyesight and the relief from the former strain must have
been a large factor in this improvement. But I am inclined to
think that the intervals of quiet and peace were wonderfully
beneficial. and why shouldn't they be? We are living on stimulants,
physical stimulants, mental stimulants of all kinds. The
minute these stop we feel we are merely existing, and yet, if we
retain any of the normality of our youth, do you not think that we
respond very happily to natural simple things ?"
RELIEF
AFTER TWENTY-FIVE YEARS
While
many persons are benefited by the accepted methods of treating
defects of vision, there is a minority of cases, known to every eye
specialist, which gets little or no help from them. These patients
sometimes give up the search for relief in despair, and sometimes
continue it with surprising pertinacity, never being able to abandon
the belief, in spite of the testimony of experience, that somewhere
in the world there must be some one with sufficient skill to fit them
with the right glasses. The rapidity with which these patients
respond to treatment by relaxation is often very dramatic, and
affords a startling illustration of the superiority of this method to
treatment by glasses and muscle-cutting. In the following case
relaxation did in twenty-four hours what the old methods, as
practiced by a succession of eminent specialists, could not do
in twenty-five years.
The
patient was a man of forty-nine, and his imperfect sight was
accompanied by continual pain and misery, culminating twenty years
before I saw him, in a complete nervous breakdown. As he was a
writer, dependent upon his pen for a living, his condition
was a serious economic handicap, and he consulted many
specialists in the vain hope of obtaining relief. Glasses did
little,- either to improve his sight, or to relieve his discomfort,
and the eye specialists talked vaguely about disease of the
optic nerve and brain as a possible cause of his troubles. The nerve
specialists, however, were unable to do anything to relieve him. One
specialist diagnosed his case as muscular, and gave him prisms, which
helped him a little.
Later,
the same specialist, finding that all of the apparent muscular
trouble was not corrected by glasses, cut the external muscles of
both eyes. This also brought some relief, but not much. At the age of
twenty-nine the patient suffered the nervous breakdown already
mentioned. For this he was treated unsuccessfully by various
specialists, and for nine years he was compelled to live out of
doors. This life, although it benefited him, failed to restore his
health, and when he came to me on September I5, 1919, he was
still suffering from neurasthenia. His distant vision was less
than 20/40, and could not be improved by glasses. He was able to read
with glasses, but could not do so without discomfort. I
could find no symptom of disease of the brain or of the interior of
the eye. When he tried to palm he saw grey land yellow instead of
black; but he was able to rest his eyes simply by closing them, and
by this means alone he became able, in twenty-four hours, to read
diamond type and to make out most of the letters on the twenty line
of the test card at twenty feet. At the same time his discomfort was
materially relieved. He was under treatment for about six weeks, and
on October 25 he wrote as follows:
"I
saw you last on October 6, and at the end of the week, the 11th, I
started off on a ten-day motor trip as one of the officials of the
Cavalry Endurance Test for horses. The last touch of eyestrain which
affected me nervously at all I experienced on the 8th and 9th. On the
trip, though I averaged but five hours' sleep, rode all day in an
open motor without goggles and wrote reports at night by bad lights,
I had no trouble. After the third day the universal slow swing seemed
to establish itself, and I have never had a moment's discomfort
since. I stood fatigue and excitement better than I have ever done,
and went with less sleep. My practicing on the trip was necessarily
somewhat curtailed, yet there was noticeable improvement in my
vision. Since returning I have spent a couple of hours a day in
practice, and have at the same time done a lot of writing.
"Yesterday,
the 24th, I made a test with diamond type, and found that after
twenty minutes' practice I could get the lines distinct, and make out
the capital letters and bits of the text at a scant three
inches. At seven I could read it readily, though I could not see it
perfectly. This was by an average daylight - no sun. In a good
daylight I can read the newspaper almost perfectly at a normal
reading distance, say fifteen inches.
"I
feel now that I am really out of the woods. I have done night work
without suffering for it, a thing I have not done in twenty-five
years, and I have worked steadily for more hours than I have been
able to work at a time since my breakdown in 1899, all without sense
of strain or nervous fatigue. You can imagine my gratitude to you.
Not only for my own sake, but for yours, I shall leave no stone
unturned to make the cure complete and get back the child eyes which
seem perfectly possible in the light of the progress I have made in
eight weeks."
SEEKING
A MYOPIA CURE
In
spite of the emphasis with which the medical profession denies the
possibility of curing errors of refraction, there are many lay
persons who refuse to believe that they are incurable. The author of
the following statement represents a considerable class, and was
remarkable only in the persistency with which he searched for relief.
He was first seen on June 27, 1919, at which time he was thirty-two
years of age. He was wearing concave 2.50D.S. for each eye, and his
vision in each eye was 20/100 . After he had obtained almost normal
vision he wrote the following account of his experiences for Better
Eyesight:
"When
the Lusitania was sunk I knew that the United States was going to get
into trouble, and I wanted to be in a position to join the Army. But
I was suffering from a high degree of myopia, and I knew they
wouldn't take me with glasses. Later on they took almost anyone who
wasn't blind, but at that time I couldn't possibly have measured up
to the standard. So I began to look about for a cure. I tried
osteopathy, but didn't go very far with it. I asked the optician who
had been fitting me with glasses for advice, - but he said that
myopia was incurable. I dismissed the matter for a time, but I didn't
stop thinking about it. I am a farmer, and I knew from the experience
of outdoor life that health is the normal condition of living beings.
I knew that when health is lost it can often be regained. I knew
that when I first tried to lift a barrel of apples onto a wagon I
could not do so, but that after a little practice I became able to do
it easily, and I did not see why, if one part of the body could be
strengthened by exercise, others could not be strengthened also. I
could remember a time when I was not myopic, and it seemed to me that
if a normal eye could become myopic, it ought to be possible for a
myopic eye to regain normality. After a while I went back to the
optician and told him that I was convinced that there must be some
cure for my condition. He replied that this was quite impossible,
as everyone knew that myopia was incurable. The assurance with which
he made this statement had an effect upon me quite the opposite of
what he intended, for when he said that the cure of myopia was
impossible I knew that it was not, and I resolved never to give up
the search for a cure until I found it. Shortly after I had the good
fortune to hear of Dr. Bates, and lost no time in going to see him.
At the first visit I was able, just by closing and resting my eyes,
to improve my sight considerably for the Snellen test card, and after
a few months of intermittent treatment I became able to read
20/10 - in flashes. I am still improving, and when I can see a little
better I mean to go back to that optician and tell him what I think
of his ophthalmological learning."
FACTS
VERSUS THEORIES
Reading
fine print is commonly supposed to be an extremely dangerous
practice, and reading print of any kind upon a moving vehicle is
thought to be even worse. Looking away to the distance, however, and
not seeing anything in particular is believed to be very beneficial
to the eyes. In the light of these superstitions the facts contained
in the following letter are particularly interesting:
"On
reaching home Monday morning I was surprised and pleased at the
comments of my family regarding the appearance of my eyes. They all
thought they looked so much brighter and rested, and that after two
days of railroading. I didn't spare my eyes in the least on the way
home. I read magazines and newspapers, looked at the scenery; in
fact, used my eyes all the time. My sight for the near-point is
splendid. Can read for hours without tiring my eyes. I went downtown
to-day and my eyes were very tired when I got home. The fine print on
the card [diamond typed] helps me so much I would like to have your
little Bible [a photographic reduction of the Bible with type much
smaller than diamond]. I'm sure the very fine print has-a soothing
effect on one's eyes, regardless of what my previous ideas on the
subject were."
It
will be observed that the eyes of this patient were not tired by her
two days railroad journey, during which she read constantly; they
were not tired by hours of reading after her return; they were rested
by reading extremely fine print; but they were very much tired by a
trip downtown during which they were not called upon to focus upon
small objects. Later a leaf from the Bible was sent to her, and she
wrote:
"The
effect even of the first effort to read it was wonderful. If you will
believe it, I haven't been troubled having my eyes feel 'crossed'
since, and while my actual vision does not seem to be any better, my
eyes feel a great deal better."
CURED
WITHOUT PERSONAL ASSISTANCE
I
am constantly hearing of patients who have been able to improve their
sight by the aid of information contained in my publications, without
personal assistance. The writer of the following letter, a
physician, is a remarkable example of these cases, as he was
able not only to cure himself, but to relieve some very serious cases
of defective vision among his patients.
"I
first tried central fixation on myself and had marvelous results. I
threw away my glasses and can now see better than I have ever done. I
read very fine type (smaller than newspaper type) at a distance
of six inches from the eyes, and can run it out at full arm's length
and still read it without blurring the type. "I have instructed
some of my patients in your methods, and all are getting results. One
case who has a partial cataract of the left eye could not see
anything on the Snellen test card at twenty feet, and could see the
letters only faintly at ten feet. Now she, can read 20/10 with both
eyes together, and also with each eye separately; but the left
eye seems, as she says, to be looking through a little fog. I could
cite many other cases that have been benefited by central fixation,
but this one is the most interesting to me."
THE
CURE OF IMPERFECT SIGHT BY
TREATMENT WITHOUT GLASSES
CHAPTER
XXXII
REASON AND AUTHORITY
Some
one - perhaps it was Bacon - has said: "You cannot by reasoning
correct a man of ill opinion which by reasoning he never acquired."
He might have gone a step further and stated that neither by
reasoning, nor by actual demonstration of the facts, can you convince
some people that an opinion which they have accepted on authority is
wrong.
A
man whose name I do not care to mention, a professor of
opththalmology, and a writer of books well known in this country and
in Europe, saw me perform the experiment illustrated on page 40, an
experiment which, according to others who witnessed it,
demonstrates beyond any possibility of error that the lens is not a
factor in accommodation. At each step of the operation he testified
to the facts; yet at the conclusion he preferred to discredit the
evidence of his senses rather than accept the only conclusion
that these facts admitted.
First
he examined the eye of the animal to be experimented upon, with
the retinoscope, and found it normal, and the fact was written down.
Then the eye was stimulated with electricity, and he testified that
it accommodated. This was also written down. I now divided the
superior oblique muscle, and the eye was again stimulated with
electricity. The doctor observed the eye with the retinoscope when
this was being done and said: "You failed to produce
accommodation." This fact, too, was written down. The doctor now
used the electrode himself, but again failed to observe
accommodation, and these facts were written down. I now sewed the cut
ends of the muscle together, and once more stimulated the eye with
electricity. The doctor said, "Now you have succeeded in
producing accommodation," and this was written down. I now
asked:
"Do
you think that superior oblique had anything to do with producing
accommodation ?"
"Certainly
not," he replied.
"Why
?" I asked.
"Well,"
he said, "I have only the testimony of the retinoscope; I am
getting on in years, and I don't feel that confidence in my ability
to use the retinoscope that I once had. I would rather you
wouldn't quote me on this."
While
the operation was in progress, however, he gave no indication
whatever of doubting his ability to use the retinoscope. He was very
positive, in fact, that I had failed to produce accommodation after
the cutting of the oblique muscle, and his tone suggested that
he considered the failure ignominious. It was only after he found
himself in a logical trap, with no way out except by discrediting his
own observations, that he appeared to have any doubts as to
their value.
Patients
whom I have cured of various errors of refraction have frequently
returned to specialists who had prescribed glasses for them, and, by
reading fine print and the Snellen test card with normal vision,
have demonstrated the fact that they were cured, without in any way
shaking the faith of these practitioners in the doctrine that such
cures are impossible.
The
patient with progressive myopia whose case was mentioned in Chapter
XV returned after her cure to the specialist who had prescribed her
glasses, and who had said not only that there was no hope of
improvement, but that the condition would probably progress
until it ended in blindness, to tell him the good news which, as an
old friend of her family, she felt he had a right to hear. But while
he was unable to deny that her vision was, in fact, normal without
glasses, he said it was impossible that she should have been cured of
myopia, because myopia was incurable. How he reconciled this
statement with his former patient's condition he was unable to make
clear to her.
A
lady with compound myopic astigmatism suffered from almost constant
headaches which were very much worse when she took her glasses off,
The theatre and the movies caused her so much discomfort that
she feared to indulge in these recreations. She was told to take off
her glasses and advised, among other things, to go to the movies; to
look first at the corner of the screen, then off to the dark, then
back to the screen a little nearer to the center, and so forth. She
did so, and soon became able to look directly at the pictures without
discomfort. After that nothing troubled her. One day she called
on her former ophthalmological adviser, in the company of a friend
who wanted to have her glasses changed, and told him of her cure. The
facts seemed to make no impression on him whatever. He only laughed
and said, "I guess Dr. Bates is more popular with you than I
am."
Sometimes
patients themselves, after they are cured, allow themselves to be
convinced that it was impossible that such a thing could have
happened, and go back to their glasses. This happened in the case of
a patient already mentioned in the chapter on Presbyopia, who was
cured in fifteen minutes by the aid of his imagination. He was very
grateful for a time, and then he began to talk to eye specialists
whom he knew and straightway grew skeptical as to the value of what I
had done for him. One day I met him at the home of a mutual friend,
and in the presence of a number of other people he accused me of
having hypnotized him, adding that to hypnotize a patient without his
knowledge or consent was to do him a grievous wrong. Some of the
listeners protested that whether I had hypnotized him or not, I
had not only done him no harm but had greatly benefited him, and he
ought to forgive me. He was unable, however, to take this view
of the matter. Later he called on a prominent eye specialist who told
him that the presbyopia and astigmatism from which he had suffered
were incurable, and that if he persisted in going without his
glasses he might do himself great harm. The fact that his sight was
perfect for the distance and the near-point without glasses had no
effect upon the specialist, and the patient allowed himself to
be frightened into disregarding it also. He went back to his glasses,
and so far as I know has been wearing them ever since. The story
obtained wide publicity, for the man had a large circle of friends
and acquaintances; and if I had destroyed his sight I could scarcely
have suffered more than I did for curing him.
Fifteen
or twenty years ago the specialist mentioned in the foregoing
story read a paper on cataract at a meeting of the
ophthalmological section of the American Medical Association in
Atlantic City, and asserted that anyone who said that cataract could
be cured without the knife was a quack. At that time I was assistant
surgeon at the New York Eye and Ear Infirmary, and it happened that I
had been collecting statistics of the spontaneous cure of cataract at
the request of the executive surgeon of this institution, Dr. Henry
G. Noyes, Professor of Ophthalmology at the Bellevue Hospital Medical
School. As a result of my inquiry I had secured records of a
large number of cases which had recovered, not only without the
knife, but without any treatment at all. I also had records of cases
which I had sent to Dr. James E. Kelly of New York and which he had
cured, largely by hygienic methods. Dr. Kelly is not a quack, and at
that time was Professor of Anatomy in the New York Post Graduate
Medical School and Hospital and attending surgeon to a large city
hospital. In the five minutes allotted to those who wished to discuss
the paper, I was able to tell the audience enough about these cases
to make them want to hear more. My time was, therefore, extended,
first to half an hour and then to an hour. Later both Dr. Kelly and
myself received many letters from men in different parts of the
country who had tried his treatment with success. The man who wrote
the paper had blundered, but he did not lose any prestige because of
my attack, with facts, upon his theories. He is still a prominent and
honored ophthalmologist, and in his latest book he gives no hint of
having ever heard of any successful method of treating cataract other
than by operation. He was not convinced by my record of spontaneous
cures, nor by Dr. Kelly's record of cures by treatment; and while a
few men were sufficiently impressed to try the treatment recommended,
and while they obtained satisfactory results, the facts made no
impression upon the profession as a whole, and did not modify the
teaching of the schools. That spontaneous cures of cataract do
sometimes occur cannot be denied; but they are supposed to be
very rare, and any one who suggests that the condition can be cured
by treatment still exposes himself to the suspicion of being a quack.
Between
1886 and 1891 I was a lecturer at the Post Graduate Hospital and
Medical School. The head of the institution was Dr. D. B. St. John
Roosa. He was the author of many books, and was honored and
respected by the whole medical profession. At the school they
had got the habit of putting glasses on the nearsighted doctors, and
I had got the habit of curing them without glasses. It was naturally
annoying to a man who had put glasses on a student to have him
appear at a lecture without them and say that Dr. Bates had cured
him. Dr. Roosa found it particularly annoying, and the trouble
reached a climax one evening at the annual banquet of the faculty
when, in the presence of one hundred and fifty doctors, he suddenly
poured out the vials of his wrath upon my head. He said that I was
injuring the reputation of the Post Graduate by claiming to cure
myopia. Every one knew that Donders said it was incurable, and I had
no right to claim that I knew more than Donders. I reminded him that
some of the men I had cured had been fitted with glasses by himself.
He replied that if he had said they had myopia he had made a
mistake. I suggested further investigation. "Fit some more
doctors with glasses for myopia," I said, "and I will cure
them. It is easy for you to examine them afterwards and see if the
cure is genuine." This method did not appeal to him, however. He
repeated that it was impossible to cure myopia, and to prove that it
was impossible he expelled me from the Post Graduate, even the
privilege of resignation being denied to me.
The
fact is that, except in rare cases, man is not a reasoning being. He
is dominated by authority, and when the facts are not in accord with
the view imposed by authority, so much the worse for the facts.
They may, and indeed must, win in the long run; but in the meantime
the world gropes needlessly in darkness and endures much
suffering that might have been avoided.